
![]() Contributed by Ryan A. Collins, MD and Marie DeFrances, MD, PhD
Contributed by Ryan A. Collins, MD and Marie DeFrances, MD, PhD
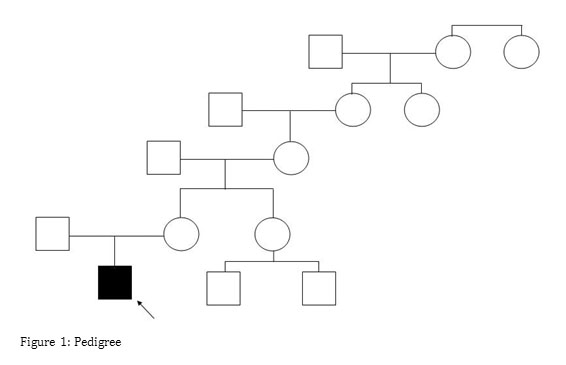
The patient is a 3 year old male who initially presented with seizures at age 18 months and was diagnosed with a Chiari malformation; this was successfully surgically repaired. During the pre-operative assessment, however, he was found to have isolated hepatomegaly. Since that time, his parents have noted increasing fatigue, leg pain, intermittent abdominal pain, and a possible two pound weight loss. Repeated blood sugar measurements revealed glucose levels in the 30s and 40s in the morning and early afternoon. He has no history of jaundice, or pruritus. There is no family history of similar symptoms (see Figure 1).
Physical exam was significant for hepatomegaly, with the liver edge palpable 3 cm below the costal margin. There is no splenomegaly, ascites, peripheral edema, or cutaneous evidence of chronic liver disease. Physical exam was otherwise unremarkable.
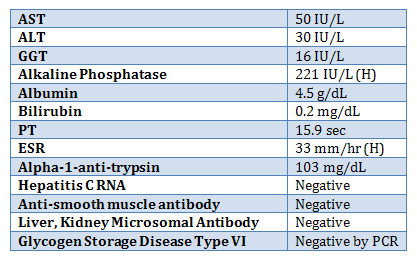
Laboratory studies were as follows:
Abdominal MRI revealed hepatomegaly with no focal abnormalities.
To further define the pathologic process, a liver biopsy was performed and demonstrated:
HEPATOCELLULAR BALLOONING WITH INTRACYTOPLASMIC LIPID AND GLYCOGEN ACCUMULATION
---- MILD PORTAL AND PERI-PORTAL FIBROSIS
As glycogen storage disease (GSD) type VI was previously excluded, the clinical team requested that we start testing for type IX GSD. Testing for phosphorylase B kinase, alpha subunit (PHKA2), with reflex testing for the beta subunit (PHKB) was requested. 3ml of blood in EDTA was received for testing.
Out of further clinical concern, prior to the return of the PHKA2 results, further molecular testing for GSD III was ordered. Testing for fructose 1,6 bisphosphatase (FBP1) , Aldolase B (ALDOB), and Amylo-alpha-1, 6-glucosidase, 4-alpha-glucanotransferase (AGL) was also performed.