![]() Contributed by Marie C. DeFrances, MD, PhD and A. Julio Martinez, MD
Contributed by Marie C. DeFrances, MD, PhD and A. Julio Martinez, MD
![]() Published on line in November1999
Published on line in November1999
PATIENT HISTORY:
The patient is a 48-year-old Caucasian woman who was in good health until approximately one week prior to presentation. She developed diffuse headache and neck stiffness as well as diplopia. The headaches gradually worsened. She presented to her primary care physician and was prescribed Zomig without relief. On the day of presentation to the emergency department, she became acutely confused and was found by her significant other to be wandering about the house. She did not recognize him and was seen to have a new bruise over the left side of her face. The patient's medications included Synthroid with questionable compliance, Zomig and Lorazepam. She had no known allergies. Past medical/surgical history revealed a history of thyroid cancer diagnosed and treated with surgical resection in 1982. Family history was positive for Sj÷gren's syndrome and lymphoma in her mother and colon cancer in her father. Review of systems was positive for impaired upward gaze and "hazy" vision. No gait disturbances, intellect changes or other focal neurological problems were identified. On physical examination, the patient was oriented to self and place; however, she remained somewhat confused during elicitation of history. Short term memory was impaired; she recalled one of five words at five minutes. Her vital signs were within normal limits. Relevant physical findings included 1+ papillaedema. Neurological examination was positive for limited right lateral gaze, light-near dissociation and convergence bias. Reflexes were depressed bilaterally, and gait was ataxic. A CT scan, a cerebrospinal fluid, and a MRI were obtained; she then underwent surgery.
LABORATORY VALUES:
On presentation, the laboratory values were: Na - 131 mEq/L, K - 3.8 mEq/L, Cl - 83 mEq/L, HCO3 - 28 mEq/L, Blood Urea Nitrogen (BUN) - 14 mg/dl, Creatinine (Cr) - 0.6 mg/dl, Glucose (Glu) - 102 mg/dl, White Blood Cell Count (WBC) - 15,100/cu mm with a differential of 91% polymorphonuclear leukocytes, 6% monocytes and 3% lymphocytes, thyroxin - 7.8 ng/dl, thyroid stimulating hormone - 3.14 ÁU/ml.
Cerebrospinal fluid yielded the following values: Glu - 52 mg/dl, Protein - 93 g/dl, Red Blood Cells (RBCs) - 4910, lymphocytes - 20, polymorphonuclear leukocytes - 32, monocytes - 44
RADIOLOGIC IMAGING:



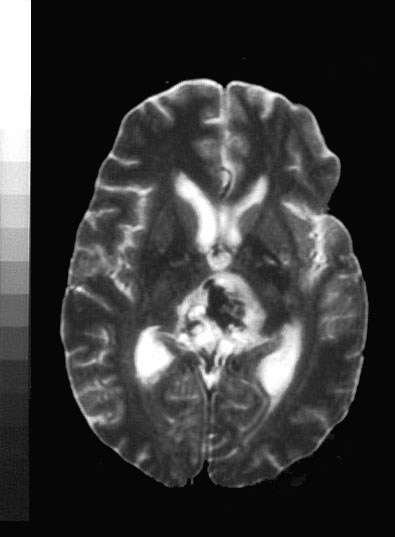
CT images without contrast demonstrated an abnormal lucency within the periaqueductal region (IMAGE 1) leading to hydrocephalus (IMAGE 2) . MRI images showed a 2.5-cm mass in the pineal region and the roof of the fourth ventricle (IMAGE 3 and IMAGE 4), which enhanced irregularly. Enhancement of the ependyma along the third ventricle as well as along the tectum was seen . Pial enhancement involving the perimesencephalic region of the parietal lobe was also noted. Hydrocephalus with enlargement of the lateral ventricles was identified.
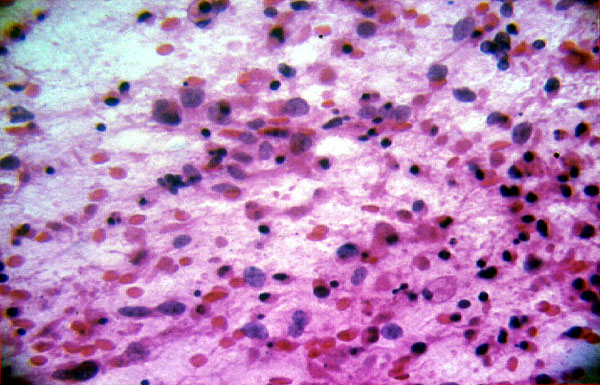
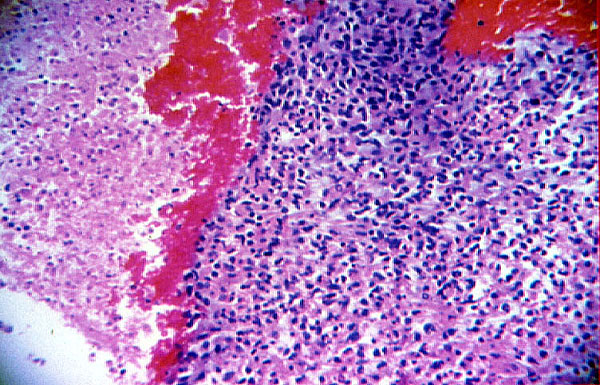
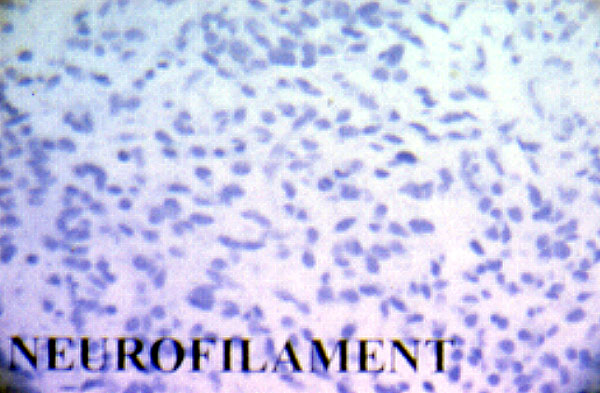
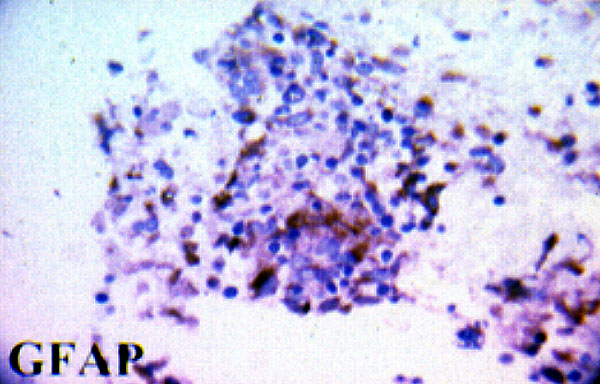
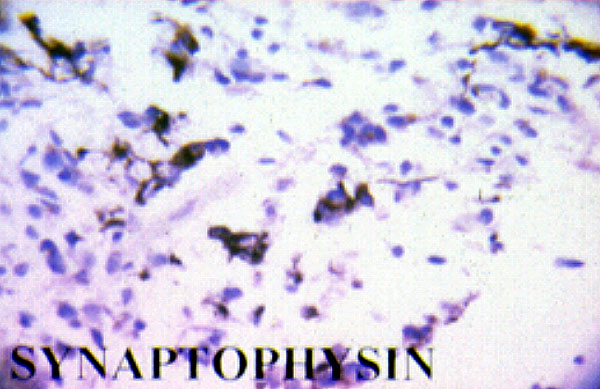
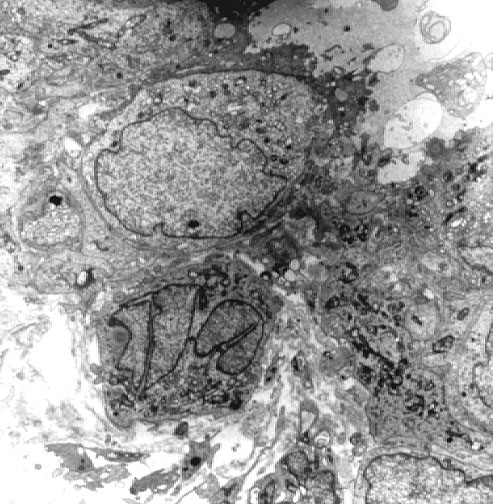
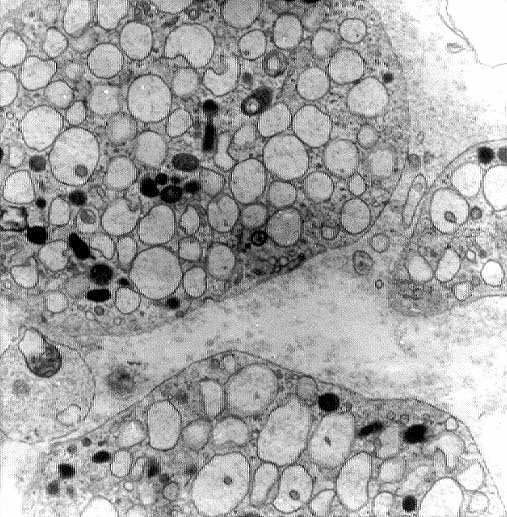
INTRAOPERATIVE MICROSCOPIC DESCRIPTION