


 PAS/D
PAS/D
MICROSCOPIC DESCRIPTION:
PAS/D
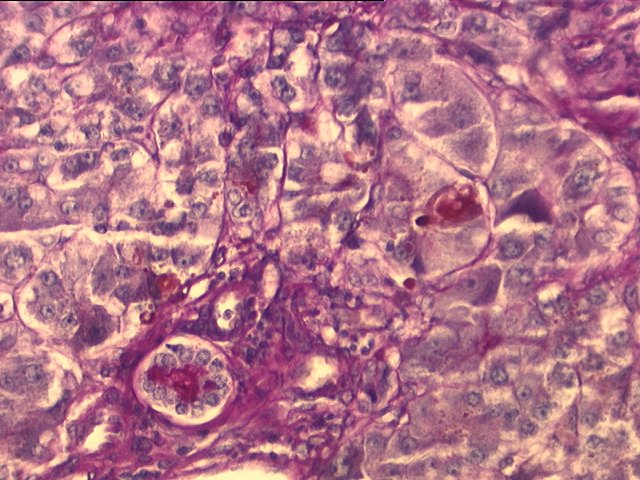
Sections through the liver show distorted hepatic architecture due to confluent bridging necrosis in varying central-central, portal-central, and portal-portal patterns. Early bridging fibrosis linking portal tracts is focally appreciated. The portal tracts contain a mild to moderate mixed (lymphoplasmacytic and neutrophilic) infiltrate with occasional eosinophils. The bile ducts demonstrate mild reactive changes, represented by epithelial atypia, vacuolization and focal acute cholangiolitis. The lobules are characterized by extensive macro- and microvesicular steatosis, moderate hepatocanalicular cholestasis, hepatocellular swelling, and Kupffer cell hypertrophy. Regenerative liver cell changes with increased N/C ratio and conspicuous nucleoli are seen. The most striking features in the sections are seen in the central vein areas. These comprise centrilobular hepatocellular dropout, hemorrhage, lymphocytic inflammation and central vein endothelialitis. Other central veins show mild to moderate fibrosis. No viral inclusions are appreciated. The regenerative nodules grossly described (sections G and H) demonstrate similar regenerative features but with more conspicuous cholestasis. No evidence of dysplasia is appreciated. In section 1D (superficial hilum), the branch of the hepatic artery shows mild fibrointimal hyperplasia, and the portal vein is essentially unremarkable. In section 1E (deep hilum), the hepatic duct and the periductular glands demonstrate focally injured epithelium with vacuolated or eosinophilic cytoplasm and reactive nuclei with conspicuous nucleolus. This is associated with periductular edema and mixed (predominantly neutrophilic) inflammation. The gallbladder shows mild mural thickening, hemorrhage, and mild mixed inflammation. Although no specific diagnostic clues to the cause of the extensive hepatic necrosis are recognized, the various changes are more suggestive of an acute toxic or drug-induced insult rather than viral hepatitis.