KASABACH-MERRITT SYNDROME WITH LOCALIZED INTRAVASCULAR COAGULATION.
CONTRIBUTORS NOTE:
Hemangiomas have been associated with a consumptive coagulopathy since Kasabach and Merritt described the case of a young infant with an extensive hemangioma who developed thrombocytopenia and a hemorrhagic diathesis in 1940.1 The consumptive coagulopathy known as Kasabach-Merritt Syndrome has been described in numerous patients with large hemangiomas (most greater than 5 centimeters in size).2,3,4,5 The patient described herein had laboratory values revealing severe thrombocytopenia, prolongation of prothrombin time, extreme prolongation of partial thromboplastin time, severe hypofibrinogenemia, elevation of fibrin degradation products, D-dimer elevation, and decreased factors II, V, VIII, IX, X, and XI. These are consistent with a consumptive coagulopathy probably best described as a localized intravascular coagulation due to the lack of other signs and symptoms at the time of laboratory testing.
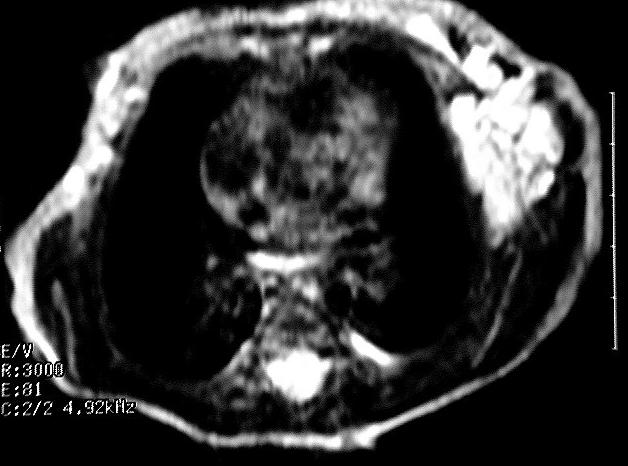


Hemangiomas are common tumors affecting infants and usually are identified in the first month of life. While usually small and innocuous, these lesions may be large and grow extensively during a proliferative phase during the first year of life.6 In this patient, an MRI performed on admission showed enlargement of the hemangioma to involve the left lower chest wall, left abdominal wall, pelvis, and left lower extremity. During an extensive hospital stay, the hemangioma extended into the patients left axilla. Following the proliferative phase which lasts approximately 6 to 10 months, the hemangioma will enter an involuting phase.6 According to Fishman and Mulliken, half the lesions will resolve by 5 years of age with most of the remaining lesions resolving by 10 to 12 years of age.6
Localized intravascular coagulation is characterized by a pattern of thrombocytopenia, hypofibrinogenemia, elevated fibrin degradation products and consumption of coagulation factors, much like its systemic counterpart disseminated intravascular coagulation. Intravascular coagulation in its localized form is associated with decreased platelet survival and consumption of fibrinogen that have been shown to accumulate in the lesion.7,8 This form of coagulopathy is not restricted to pediatric patients with hemangiomas, and a similar hemorrhagic disorder has been reported in patients with aortic aneurysms and renal allograft rejection.9,10
REFERENCES:
- Kasabach, HH., Merritt, KK: Capillary haemangiomas with extensive purpura. American Journal of Diseases of Childhood. 59:1063-70, 1940.
- Furman G, Sills J, Zeltzer P, Warden J. Perinantal/Neonatal Casebooks: Kasabach-Merritt Syndrome. Journal of Perinatology. 15:242-245, 1995.
- Rodrigues-Erdmann F, Button L, Murray JE, Moloney WC. Kasabach-Merritt syndrome: coagulo-analytical observations. The American Journal of the Medical Sciences. 261: 9-15, 1971.
- Henley JD, Danielson CF, Rothenberger SS, et al. Kasabach-Merritt Syndrome with Profound Platelet Support. American Journal of Clinical Pathology. 99: 628-630, 1992.
- Esterly NB. Kasabach-Merritt Syndrome in Infants. Journal of the American Academy of Dermatology. 8:504-512, 1983.
- Fishman, S., Mulliken, J. Hemangiomas and Vascular Malformations of Infancy and Childhood. Pediatric Clinics of North America. 40:1177-1200, 1993.
- Straub, PW, Kessler S, Schreiber A, et al. Chronic intravascular coagulation in Kasabach-Merritt Syndrome: Preferential accumulation of fibrinogen 131I in a giant hemangioma. Archives of Internal Medicine. 129:475, 1972.
- Hoak JC, Warner ED, Cheng HF et al: Hemangioma with thrombocytopenia and microangiopathic anemia (Kasabach-Merritt Syndrome): An animal model. Journal of Laboratory Clinical Medicine. 77:941, 1971.
- Fine NL, Applebaum J,Elguezabal A, et al. Multiple coagulation defects in association with dissecting aneurysm: Archives of Internal Medicine 119: 522, 1967.
- Clarkson AR, Morton JB, Cash JD. Urinary fibrin/fibrinogen degradation products after renal homotransplantation. Lancet. 2:1220, 1970.
![]() Contributed by Christine Dorvault, M.D. and Franklin Bontempo, M.D.
Contributed by Christine Dorvault, M.D. and Franklin Bontempo, M.D.