
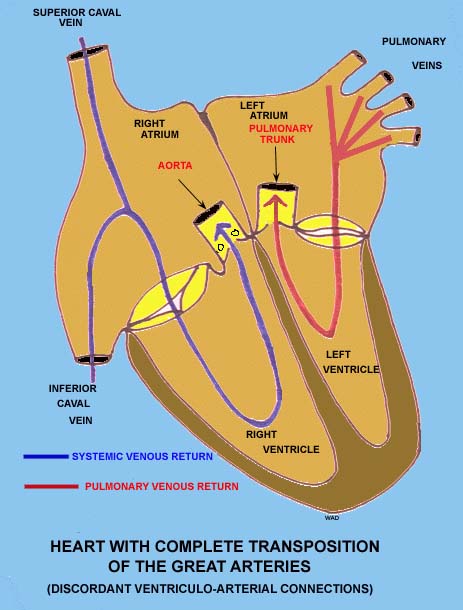
Complete (D) transposition of the great vessels refers to complete morphological reversal of the aorta and the pulmonary artery. This produces a circulation which is completely pulmonary on one side and completely systemic on the other (i.e., they are operating in parallel). Without a preexisting defect such as a ventricular septal defect or a persistent ductus arteriosus to allow for some mixing of systemic and pulmonary circulations, life cannot be sustained. "Corrected" (L) type transposition describes a condition in which the normal pattern of circulation is intact, but the left and right ventricles are switched. This produces a situation in which an intrinsically weaker muscle (the right ventricle) is forced to sustain a systemic blood pressure, and the stronger left ventricle forces blood through the pulmonary tree at a relatively higher flow pressure which is deleterious to the delicate pulmonary vascular tree. Thus, this condition will present clinically in a similar fashion to type D transposition, with cyanosis and peripheral hypoxemia and severe progressive pulmonary hypertension. Other variants of these transpositions exist, such as double outlet ventricle (in which both great vessels arise from one or the other ventricle), otherwise known as a partial transposition. A rare variant, known as truncus arteriosus, has an incomplete or absent separation of the great vessels from their embrylogical common vessel, forming a single large vessel, usually overriding a large ventricular septal defect.
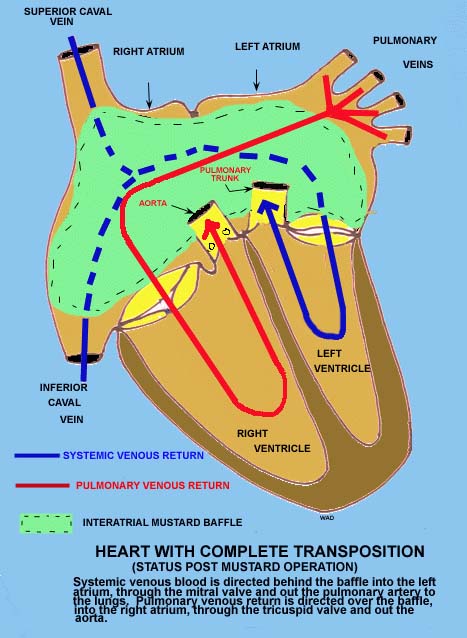
Surgical repair of transposition has been approached in several different ways in the past. Initially, grafts may have been interposed between systemic and pulmonary vessels to function as shunts to allow intercirculatory mixing and palliate the cyanotic spells and pulmonary hypertension of the disease. Corrective procedures, such as the Senning and the Mustard operations, were then adopted. These procedures respectively involved surgically switching the right and left atria (and large veins) and creating an inter-atrial shunt (or "Mustard baffle") to correct blood flow anatomically. The current procedure, the great arterial switch operation, has met with great long term success (long term mortality less than 7% in one study). The operation involves surgical switching of the aorta and the pulmonary trunk onto the anatomically correct ventricles. The coronary arteries are then reimplanted (with a surrounding rim, or "button" of aortic wall to prevent scarring or stenosis of the coronary ostia) into the reimplanted aorta which is now correctly arising from the left ventricle.
Galloway, et al. "Congenital Heart Disease" in Principles of Surgery. Schwartz, editors; McGraw Hill, 6th ed., 1994. Gravanis, et al. Cardiovascular Disorders: Pathogenesis and Pathophysiology. Mosby publishers, 1993. Kaplan, et al. "Congenital Heart Disease" in Cecil Textbook of Medicine. Wyngaarden editors, Saunders, 19th ed., 1992. Stocker, et al. Pediatric Pathology. J.B. Lippincott, 1992.
![]() Contributed by Kevin D. Horn, MD
Contributed by Kevin D. Horn, MD
![]() Photos and diagrams of the heart provided by William Devine of Children's Hospital, Pittsburgh, PA
Photos and diagrams of the heart provided by William Devine of Children's Hospital, Pittsburgh, PA