FINAL DIAGNOSIS
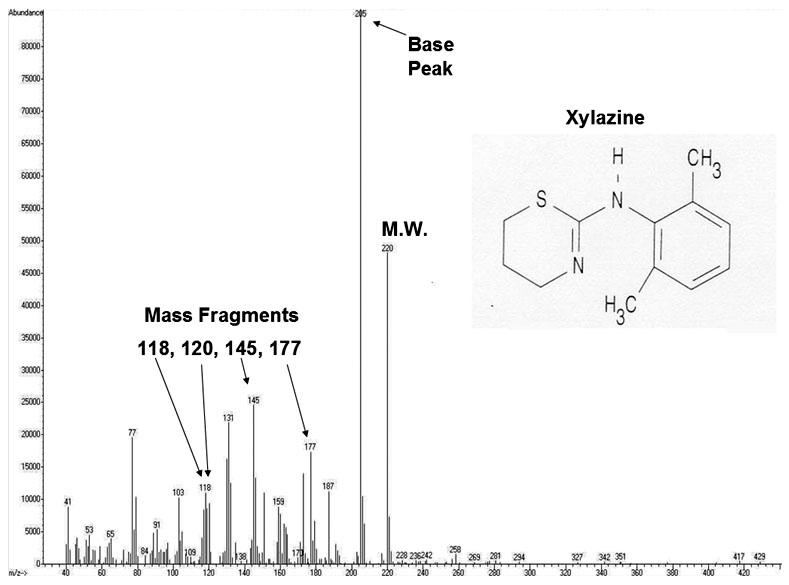
Figure 2 represents the annotated version of the mass spectrogram from Figure 1.
Neither the heroin metabolite 6-acetylmorphine nor heroin was detected. However, patient had a known history of heroine abuse. The main metabolites of heroin are 6-acetylmorphine and morphine, leaving open the possibility that heroin was consumed but not detected due to metabolism. Codeine is commonly found in heroin sold on the street. In the synthesis of heroin from opium (which contains morphine and codeine), codeine is often not completely removed in the purification and acetylation of morphine to produce heroin. Another interpretation of the test results for the case is that the patient overdosed on codeine +/- morphine.
Figure 2 demonstrates that an additional drug, xylazine, was identified by GC-MS in this patient's urine. Xylazine is an analgesic, sedative, and muscle relaxant used in the veterinary setting prior to surgical procedures. The drug is not approved for use in humans by the FDA. The drug is similar in its pharmacology to the phenothiazines and clonidine. The drug acts as a central alpha-2 agonist and may cause bradycardia and hypotension. Post-mortem examination of the urine and/or blood of drug-related deaths increased awareness of xylazine as a potential contaminant in recreational drug preparations or as a drug intentionally abused (e.g., by someone who gets access to veterinary medicine stocks). However, as in the case, it is not possible to determine the exact contribution of each compound found in a drug preparation to a patient's death.
Few reports regarding the effects of xylazine use in humans are available. One case report described a veterinary surgeon's wife with repeated bouts of tiredness, faintness, blurred vision, and sinus bradycardia who eventually admitted to taking xylazine for pain.
Another case report describes a patient who self-administered a large dose of xylazine and was subsequently found collapsed and stopped breathing. The patient apparently was on a respirator for some 60 hours until recovery.
We hope that this web case illustrates the utility of GC-MS in identifying illicit drugs which may not be picked up on initial screening. It also highlights the complex nature of interpreting the cause of death in drug overdose-related deaths.
REFERENCES
Haigh J.C. 1988. Misuse of xylazine. Can. Vet. J. 29:782-3
Lewis S. 1983. Clinical curio: self medication with xylazine. British Medical Journal 287(5):1369.
Nayra R. et al. 2008. GC-MS confirmation of xylazine (Rompun), a veterinary sedative, in exchanged needles. Drug and Alcohol Dependence 96:290-3
Pincus M.R. and Abraham N.Z. 2007. Chapter 23: Toxicology and Therapeutic Drug Monitoring. In Henry's Clinical Diagnosis and Management by Laboratory Methods, 21st Edition
Wong S.C., Curtis J.A., Wingert W.E. 2008. Concurrent detection of heroin, fentanyl, and xylazine in seven drug-related deaths reported from the Philadelphia Medical Examiner's Office. J. Forensic Sci. 53(2):495-8
![]() Contributed by Timothy S Gorrill MD, Ph.D. and Matthew D Krasowski MD, PhD
Contributed by Timothy S Gorrill MD, Ph.D. and Matthew D Krasowski MD, PhD