DISCUSSION:
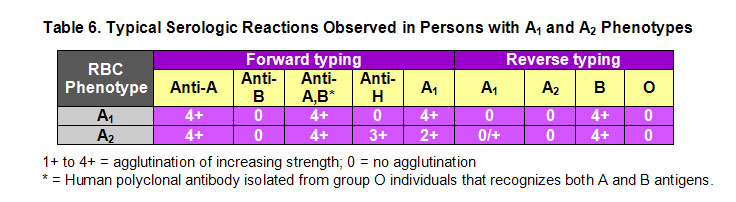
Subtypes of blood groups A and B feature diminished amounts of A and B antigens on the RBC surface and result from polymorphisms in the ABO gene. These subtype alleles encode less efficient glycosyltransferases leading to the weak A or B phenotype. A1 represents the "wild-type" A phenotype. The most common allele underlying the A2 phenotype features a frameshift mutation, which lengthens the translated protein by 21 amino acids, and renders it hypofunctional compared to the wild type A-synthesizing enzyme (Figure1). Red cells from A1 and A2 persons both react strongly with monoclonal anti-A reagents in direct agglutination tests (Table 6). Distinction between these two subgroups is made with preparations of the lectin from Dolichos biflorus seeds. The D. biflorus lectin reacts specifically with A1, and will thus agglutinate A1 but not A2 red cells.
The vast majority of group A or group AB individuals are classified as A1 or A1B since their red cells are agglutinated by D. biflorus lectin, while those individuals whose cells are strongly agglutinated by monoclonal anti-A but not by the anti-A1 lectin are considered type A2 or A2B.2 While about 20% of Caucasian blood group A or AB individuals are A2 or A2B, respectively, only about 1-2% of A2 individuals produce a naturally occurring anti-A1 whereas 22-26% of A2B individuals demonstrate an anti-A1.3 Insights as to the causes of different antibody production in A2 individuals compared to A2B individuals might be extrapolated from a 1998 study by Osagawara et al. This study of Japanese blood donors found the *R101 allele in about 1% of A2 and A1O samples while it was present in 41% of A2B samples. Competition for the ABO precursor substance, H antigen, between the *R101-encoded transferase and a normal B transferase may lead to reduced A antigen expression on the RBCs resulting in these individuals being typed as A2B. When inherited with an O allele, which does not encode a functional glycosyltransferase enzyme, the R101-encoded glycosyltransferase produces the A1 phenotype.4 In Caucasians, the A201 allele is the most common allele that gives rise to the A2 phenotype. As described for the *R101 allele in the Japanese population, individuals with an A2B phenotype are more likely to produce an anti-A1 than A2 individuals because of the relative reduction of A antigens on A2B cells. 5
Significant transfusion reactions due to anti-A1 are rare since their thermal range is typically only up to 25şC. In fact, many of the published cases that have reported a clinically significant anti-A1 antibody are in patients who had undergone cardiac surgery using cold cardioplegia.6,7
6. Given the laboratory findings, is this anti-A1 likely to be clinically significant? [ Answer ]
Additional Questions
7. How can we explain the patient's excellent response to O RBCs? [ Answer ]
8. What is your differential diagnosis for this patients' hemolysis after reading this discussion? [ Answer ]
9. What further laboratory investigations would you order? [ Answer ]
REFERENCES:
![]() Contributed by Nicole Nicosia Esposito, MD, Don Kelley, MD, Beth Jochum and Mark H Yazer, MD, FRCPC
Contributed by Nicole Nicosia Esposito, MD, Don Kelley, MD, Beth Jochum and Mark H Yazer, MD, FRCPC