
FINAL DIAGNOSIS:
CONTRIBUTOR'S NOTE:
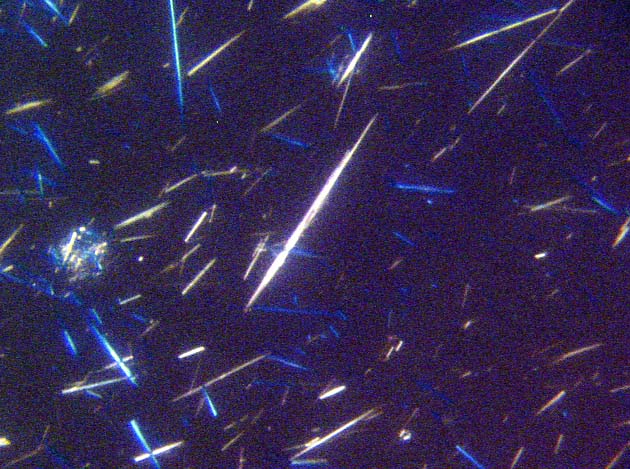
If gout is suspected in a specimen, imprint preparations made from the chalky material and visualized under polarizing microscope, will show negatively birefringent needle shaped monosodium urate crystals ( Figs 9, 10 from another case)
Gout is the common end point of a group of disorders that produce hyperuricemia. Although hyperuricemia is a sin qua non for the development of gout, it is not the sole determinant. More than 10% of the population of western hemisphere have hyperuricemia but gout develops in less than 0.5% of the population. A plasma urate level above 7 mg/dl is considered elevated because it exceeds the saturation value for urate at normal body temperature and blood pH. The various conditions producing hyperuricemia and gout are divided into those that produce primary gout in which the basic metabolic defect is unknown or gout is the main manifestation of a known defect and secondary gout in which the cause of hyperuricemia is known or gout is not the main clinical dysfunction. Most first attacks of the gouty arthritis follow 20 to 40 years of sustained hyperuricemia; The peak age of onset of gout is between 40 and 60 years for men and after menopause for women.
Our patient is a young female who was on Cyclosporine immunosuppression after her renal transplant for Polycystic kidney disease. Cyclosporine (CyA) is a potent immunosuppressive agent used in organ transplantation and autoimmune disease. Its serious side effects include nephrotoxicity, systemic hypertension and lymphoproliferative disorders. Transplanted patients under CyA have a higher incidence of hyperuricemia. This association of CyA and hyperuricemia is well established and has been reported in renal, heart transplant recipients and in patients with non transplant disease states like autoimmune uveitis. The documented incidence of CyA induced hyperuricemia is upto 80% and that of gout is 5 to 24% in renal transplant patients. Additional risk factors reported with CyA associated hyperuricemia include diuretic use, renal insufficiency and male sex. The mechanism of CyA induced hyperuricemia is complex and probably multifactorial. Recent literature favor a specific impaired tubular handling of uric acid due to CyA induced proximal tubular dysfunction.
REFERENCES