
![]() Contributed by Scott M Kulich MD, PhD and Sydney Finkelstein, MD
Contributed by Scott M Kulich MD, PhD and Sydney Finkelstein, MD
![]() Published on line in May 1999
Published on line in May 1999
PATIENT HISTORY (Part I):
The patient, a 64-year-old woman with a long history of irritable bowel syndrome, was referred to a gastroenterologist for colonoscopy to evaluate a recent exacerbation of diarrhea, increased abdominal cramping, and weight loss. Rectal examination revealed hemorrhoids. No mucosal lesions were identified on colonoscopic examination and random biopsies were taken from the descending and sigmoid colon.
GROSS DESCRIPTION (Part I):
The specimen was submitted in buffered formalin identified as "left colon" and consisted of two irregular fragments of translucent, delicate, pale tan-white tissue, 0.2 and 0.3 cm. in greatest dimension.
MICROSCOPIC DESCRIPTION (Part I):

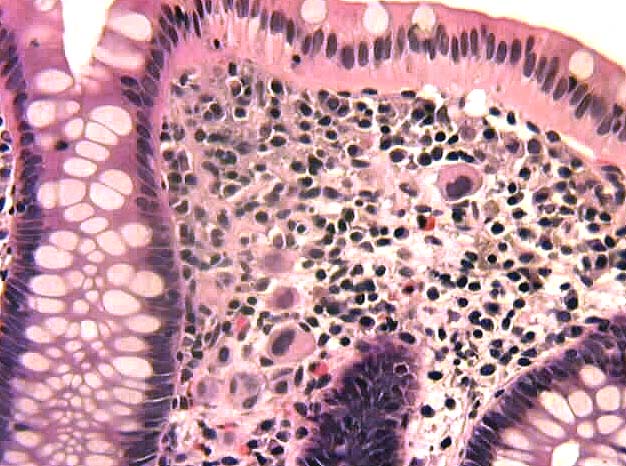
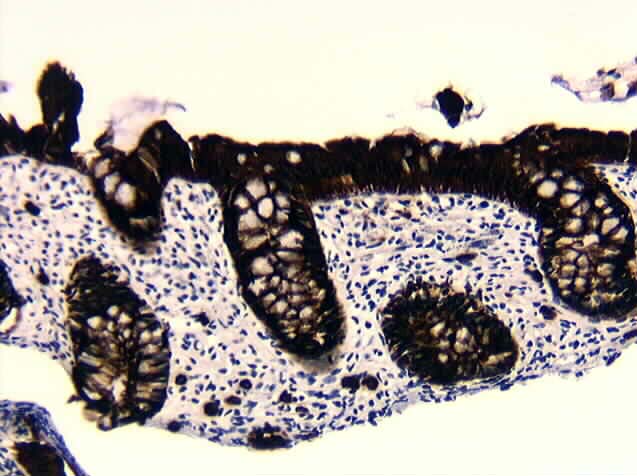

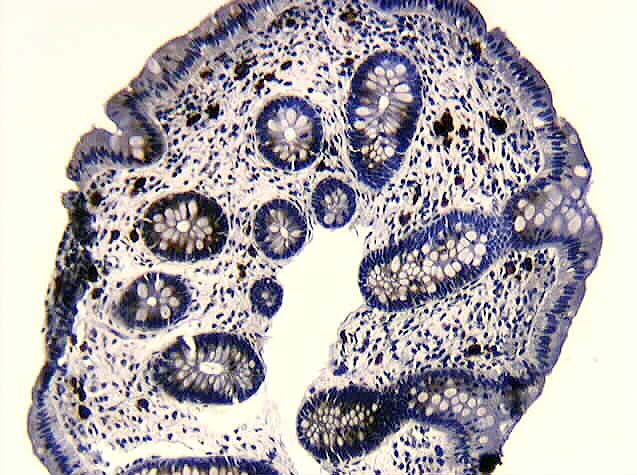
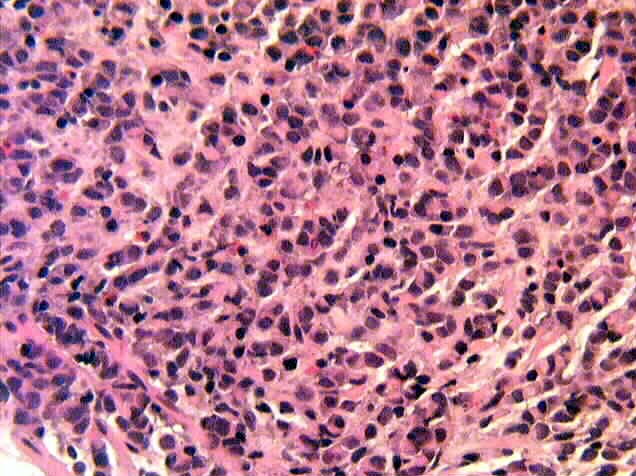
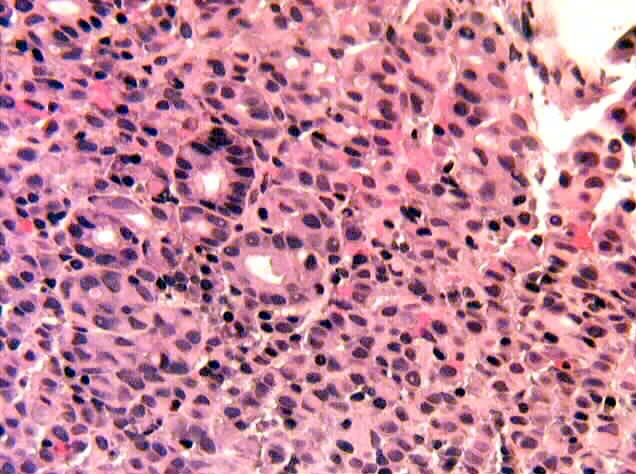
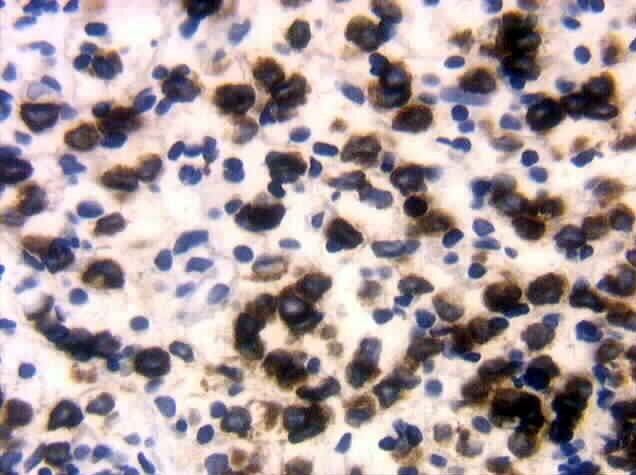
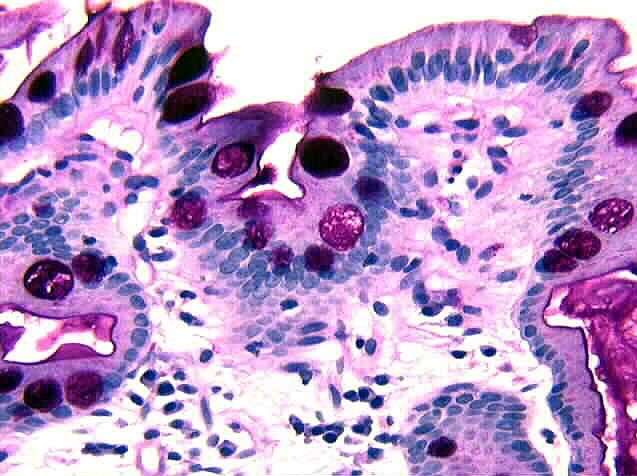
Sections revealed normal appearing colonic mucosa. The lamina propria demonstrated focal areas of increased cellularity (Figure 1). Within these areas scattered rare large atypical cells with hyperchromatic nuclei and eosinophilic cytoplasm were identified (Figure 2). Immunohistochemical stains demonstrated positive staining for cytokeratin (AE1/AE3), CEA, and EMA (Figures 3, 4 and 5) while negative staining was observed for CMV and CD68.
PATIENT HISTORY (Part II):

An EGD was performed which revealed a normal caliber esophageal lumen without a hiatus hernia. The stomach contained rugal folds of normal thickness. Focal areas of nodularity within the fundus and antrum (Figure 6) were observed and random biopsies of these areas were obtained.
GROSS DESCRIPTION (Part II):
The specimen was submitted in buffered formalin identified as "gastric antrum and fundus" and consisted of nine curled strips of tan-yellow rubbery mucosa, 0.1 to 0.4 cm. in greatest dimension.
MICROSCOPIC DESCRIPTION (Part II):
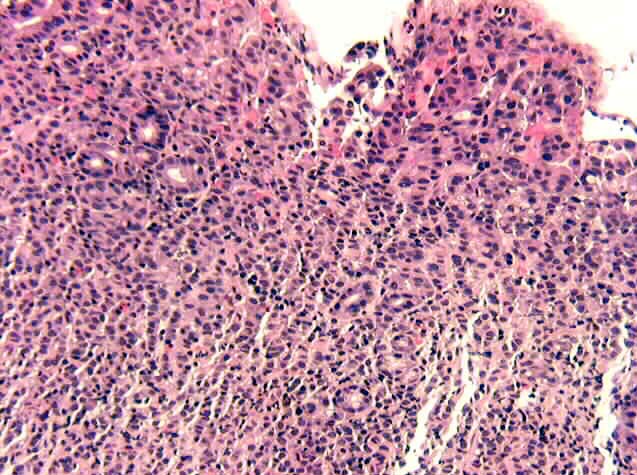
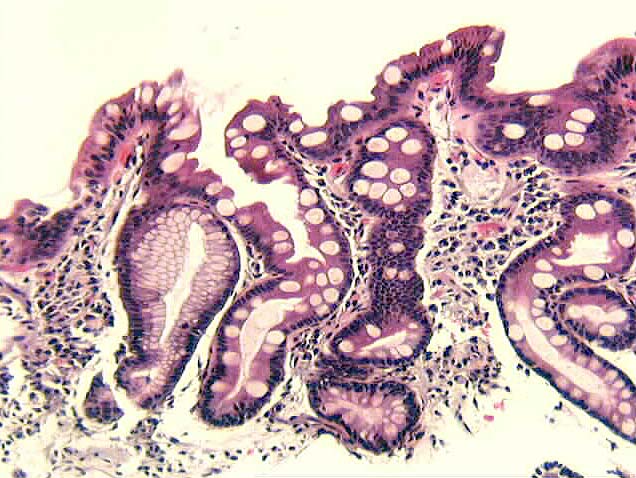
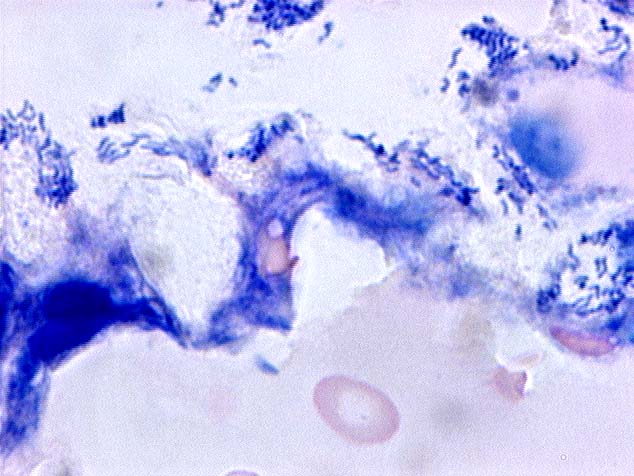
Sections revealed gastric mucosa with focal areas of disrupted architecture and superficial ulceration. In these areas the underlying lamina propria and muscularis mucosa contained collections of discohesive large cells which were similar in appearance to the atypical cells identified in the previous colonic biopsies (Figures 7 and 8). Dysplastic glands were also present (Figure 9). The epithelial nature of the infiltrating cells was confirmed by immunohistochemical staining with pankeratin (Figure 10). Other areas of the biopsy showed incomplete intestinal metaplasia containing goblet cells but lacking a well-defined brush border (Figure 11, H&E, Figure 12, PASD) as well as heavy colonization by microorganisms morphologically consistent with Helicobacter pylori (Figure 13, Giemsa,).