DIAGNOSIS: Pilocytic astrocytoma (WHO grade I) with widespread dissemination in the CNS. The diagnosis was confirmed by the German reference center for brain tumors in Bonn.
DISCUSSION:
This neuropathologically rather unproblematic case is worth consideration for several reasons. First, it is an unusual finding that a histologically benign tumor is capable of widespread dissemination within the CNS. Second, this feature is unfamiliar to clinicians and even neuropathologists so that presentation of this case leads to a greater awareness of this phenomenon helping to avoid an unnecessary delay of treatment.
Low-grade astrocytomas in children exhibit typically benign growth characteristics and have a good prognosis. In contrast to this, a small percentage of these tumors (4 %) manifest widespread dissemination either at presentation or later (2, 4, 5, 7). Astrocytomas with a predelection for cerebral spinal fluid seeding are lesions in close proximity to the ventricles and basal cisterns like in our case. In addition to a periventricular tumor location, operative manipulation has been suggested to play a role in tumor dissemination (5).
In the recently published cases of childhood astrocytoma with widely distributed cerebrospinal fluid metastases, presence of tumor dissemination was detected at a presymptomatic stage using MRI as in our case. In such cases, cytologic examination of the cerebrospinal fluid failed to demonstrate the presence of malignant cells (7). As in our case the disseminated tumor nodules showed a strong and diffuse contrast medium enhancement. Because histology of these lesions lacked anaplastic features, enhancement was not interpreted as a sign of malignancy. It might, however, be due to high densities of blood vessels. Our case indeed demonstrated high vascularity in the seeding tissue but not in the initial specimen. The reason for the difference in blood vessel content is unknown.
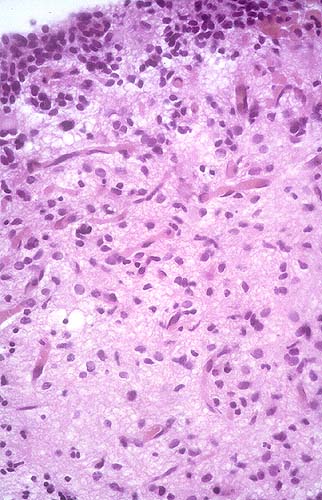
Also unknown are the factors which make benign astrocytomas capable to spread within the cerebrospinal fluid. Moreover, it is not clear whether this ability is restricted to particular neoplastic cell populations. Fig 8B shows aggregates of small tumor cells within the ventricle near the tumor surface but without connection to it suggesting that these cells might be the spreading cell population. They are identical to the cells which form the 'layers' at the ventricular site of the tumor (Fig. 8A). Whether these cells differ from the other neoplastic cells molecular genetically has not been determined at present.
The prognosis for children with dissemination of a benign astrocytoma is considerably better than that for those with disseminated malignant gliomas (3). Although histological anaplasia is lacking, children have been treated aggressively with radiotherapy and chemotherapy with good response. Under this therapeutic strategy, metastases diminished in size or did not grow further (1, 2, 5, 6). One case in a four-year old girl, however, has been reported in which under chemotherapy and radiation no further growth of tumor spreadings was noted first, whereas later numerous confluent tumor masses developed. She eventually died of central circulatory failure (8). Until now, the patient presented here has showed no progression of disease under polychemotherapy.
This case illustrates the importance of recognizing cerebrospinal fluid spread as a possible feature in benign juvenile astrocytomas, which does not inevitably mean a malignant course of the disease. In contrast, if the true benign histopathology of the metastases (or at least of one of the metastatic lesions) has been proven, prognosis is potentially good when treatment with radiation and/or chemotherapy is performed. However, cases with bad outcome have been described.
REFERENCES
![]() Contributed by Stephan Patt, Nils Haberland, Hagen Graupner, Dieter Schreiber and Rolf Kalff
Contributed by Stephan Patt, Nils Haberland, Hagen Graupner, Dieter Schreiber and Rolf Kalff
{kind=link}