LABORATORY WORKUP:
A chest radiograph revealed diffuse bilateral airspace disease and changes consistent with fluid overload. An electrocardiogram showed tachycardia, but demonstrated no evidence of ST or T wave abnormalities. Cardiac isoenzymes also showed no evidence of acute myocardial infarction. Selected laboratory tests from early in the patient's clinical course revealed the following:
| Serum Chemistry | Patient's | Normal Range |
|---|---|---|
| Na | 142 mEq/L | ( 136 - 146 ) |
| K | 2.9 mEq/L | ( 3.5 - 5.0 ) |
| Cl | 97 mEq/L | ( 95 - 110 ) |
| CO2 | 36 mEq/L | ( 21 - 31 ) |
| BUN | 70 mg/dL | ( 5 - 20 ) |
| Creatinine | 3.9 mg/dL | ( 0.5 - 1.4 ) |
| Glucose | 214 mg/dL | ( 70 - 110 ) |
| Total Protein | 6.2 g/dL | ( 6.3 - 7.7 ) |
| Albumin | 3.1 g/dL | ( 3.5 - 5.0 ) |
| Alk-Phos | 100 IU/L | ( 40 - 125 ) |
| Calcium | 12.2 mEq/L | ( 8.5 - 10.5 ) |
| Phosphate | 5.7 mEq/L | ( 2.5 - 4.5 ) |
| Uric Acid | 16.9 mg/dL | ( 2.5 - 7.5 ) |
| Complete Blood Count | Patient's | Normal Range |
|---|---|---|
| WBC | 4.7 10x9/L | ( 4.5 - 11.0 ) |
| RBC | 3.12 10x9/L | ( 3.79 - 5.23 ) |
| Hgb | 10.0 g/dL | ( 11.7 - 15.7 ) |
| Hct | 28.4 % | ( 35.0 - 47.0 ) |
| MCV | 90.8 fL | ( 80.0 - 100.0 ) |
| MCH | 31.9 pg | ( 28.2 - 32.2 ) |
| MCHC | 35.1 g/dL | ( 31.7 - 35.7 ) |
| RDW | 15.6 % | ( 11.5 - 15.0 ) |
| PLT | 55 10x9/L | ( 150 - 450 ) |
| Manual Differential | Patient's | Abs.# | Normal Range |
|---|---|---|---|
| Polys | 34% | ( 1.60 ) | ( 2.0 - 6.8 ) |
| Bands | 15% | ( 0.71 ) | ( 0.1 - 0.8 ) |
| Lymphs | 17% | ( 0.80 ) | ( 1.0 - 4.2 ) |
| Alymph | 1% | ( 0.05 ) | |
| Monos | 16% | ( 0.75 ) | ( 0.1 - 0.8 ) |
| Eos | 2% | ( 0.09 ) | ( 0.0 B 0.2 ) |
| Blasts | 13% | ( 0.61 ) | ( 0.0 B 0.02 ) |
| Myelo | 2% | ( 0.09 ) | |
| NRBC/100 WBC = 5 | |||
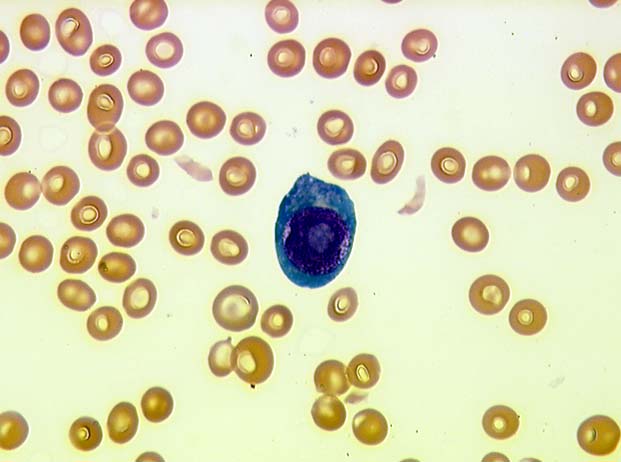
| **Blasts appear plasmacytoid**(Image 01) | |||
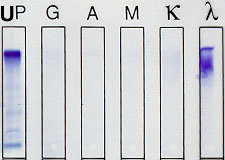
Serum and Urine Protein Electrophoresis:
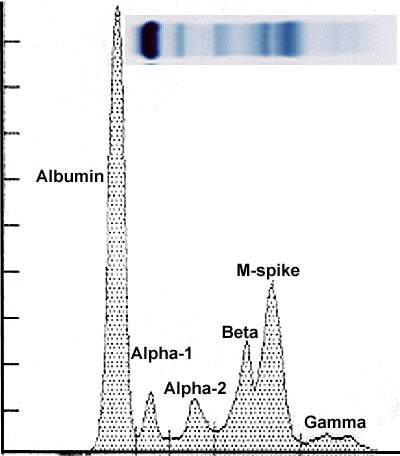
Due to the patient's renal insufficiency and low total protein and albumin, both serum and urine protein electrophoresis were performed. The serum protein electrophoresis (SPE) (Image 02) demonstrated the following:
| Normal Range | |||
|---|---|---|---|
| Total Protein | 6.80 g/dL | ( 6.00 - 8.30 ) | |
| Albumin | 45.65 % | 3.10 g/dL | ( 3.20 - 5.20 ) |
| Alpha - 1 | 5.62 % | 0.38 g/dL | ( 0.10 - 0.40 ) |
| Alpha - 2 | 7.78 % | 0.53 g/dL | ( 0.60 - 1.00 ) |
| Beta | 34.95 % | 2.38 g/dL | ( 0.60 - 1.40 ) |
| Gamma | 6.00 % | 0.41 g/dL | ( 0.70 - 1.60 ) |
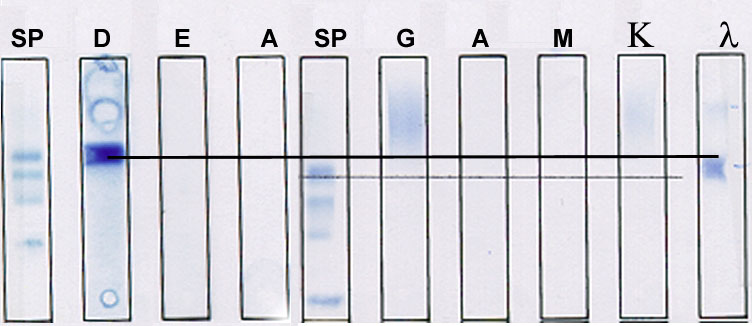
The interpretation of the SPE results was for decreased prealbumin, albumin, alpha-2, and gamma globulins; and a paraprotein spike of approximately 1.2 g/dL detected in the beta region. Serum immunofixation electrophoresis (Image 03) identified the beta region paraprotein as a monoclonal IgD/lambda.
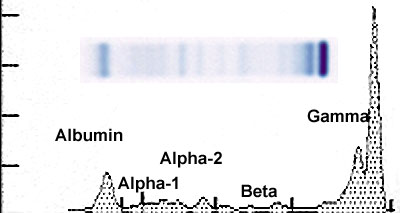
Urine protein electrophoresis (Image 04) and immunofixation electrophoresis (Image 05) demonstrated the following:
| Normal Range | |||
|---|---|---|---|
| Urine Total Protein | 104.4 mg/dL | ( < 140 mg/24hr ) | |
| Urine Albumin | 13.42 % | 14.0 mg/dL | ( < 30 mg/24hr ) |
| Urine alpha-1 | 3.00 % | 3.1 mg/dL | |
| Urine alpha-2 | 12.70 % | 13.3 mg/dL | |
| Beta-globulin | 8.40 % | 8.8 mg/dL | |
| Gamma-globulin | 62.47 % | 65.2 mg/dL |
The interpretation is consistent with a tubular pattern of proteinuria, with monoclonal free lambda light chains ( ~ 60 mg/dL ) detected in the gamma region.
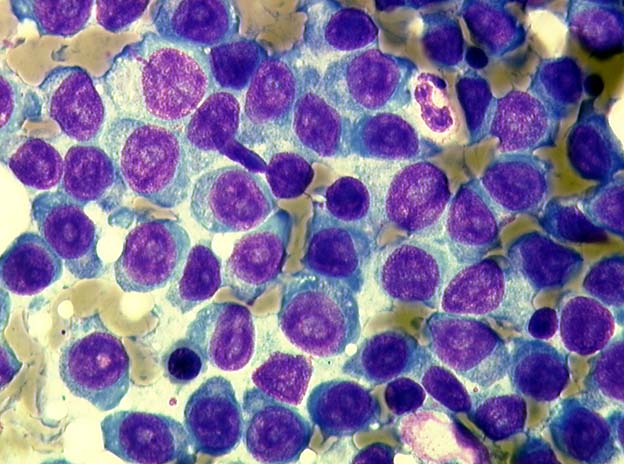
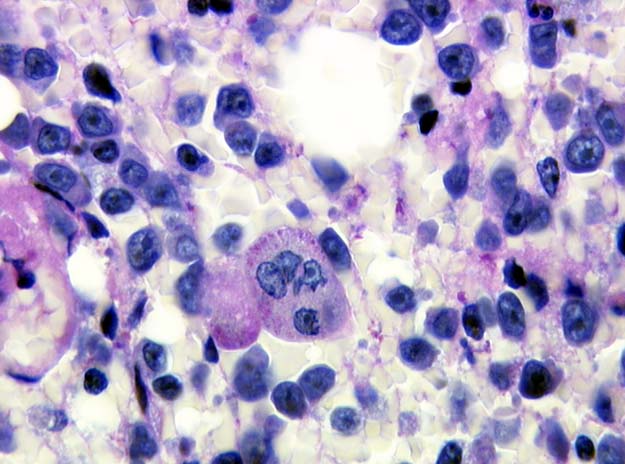
Bone Marrow Evaluation:
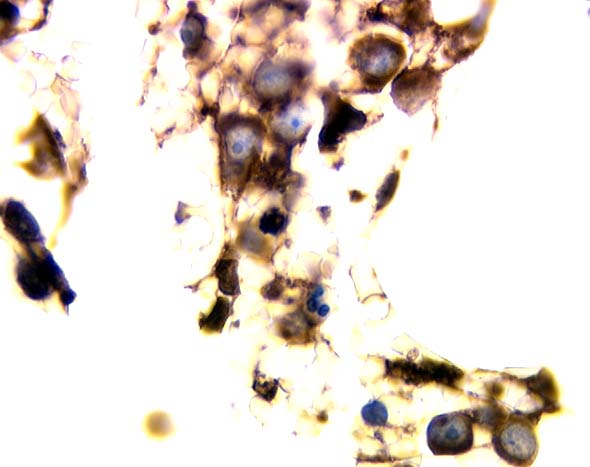
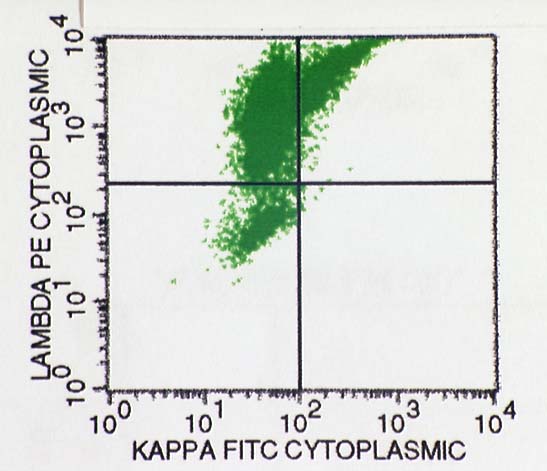
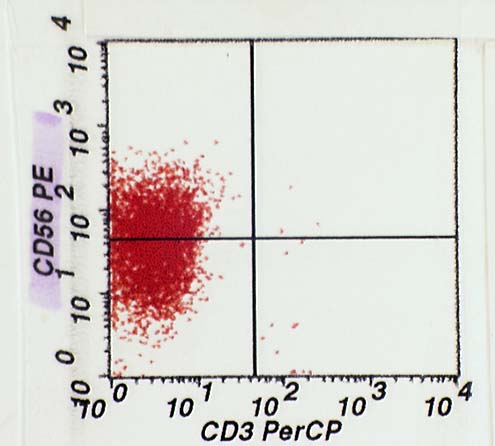
Given the presence of 13% blasts in the peripheral blood smear, and new evidence of a significant IgD paraprotein, a bone marrow biopsy and aspirate were performed to evaluate the patient's hematopoietic status. The bone marrow aspirate showed numerous blastic appearing plasmacytoid cells with prominent nucleoli and variable amounts of basophilic cytoplasm (Image 06). Overall, the bone marrow biopsy was hypercellular and almost completely replaced by a diffuse proliferation of large cells. Normal hematopoietic elements were also readily identified (note the megakaryocyte in the center of the field), but in severely decreased numbers with background stromal injury. The large blastic appearing cells showed increased nuclear-cytoplasmic ratios, and very prominent nucleoli (Image 07). Immunohistochemical stains of the biopsy section showed numerous lambda positive cells corresponding to the blast population (Image 08). These cells were kappa, CD20, and CD3 negative by immunohistochemical methods. Review of the flow cytometric histograms performed on the bone marrow, also confirmed the lambda positivity of the blast population (Image 09), which was also in part CD56 positive, a marker often expressed on plasma cells (Image 10). The plasma cell marker CD138 (B-B4), however, showed little to no positivity by flow cytometry.
Hospital Course:
The remainder of the patient's hospital course showed successful correction of the acute renal failure, severe anemia, and thrombocytopenia by fluid/electrolyte management and multiple blood product transfusions. Unfortunately, this patient remained ventilator dependent during the entire course secondary to progressive, severe adult respiratory distress syndrome. The patient ultimately expired following cardiopulmonary failure several days following admission.