



MICROSCOPIC DESCRIPTION:
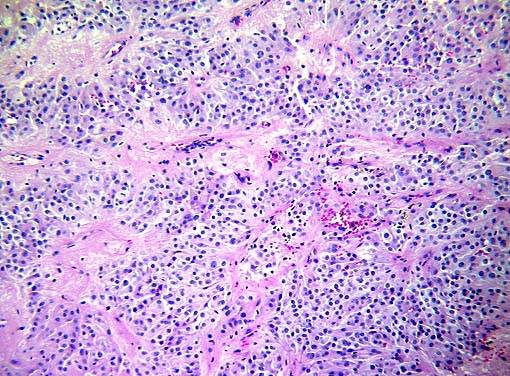
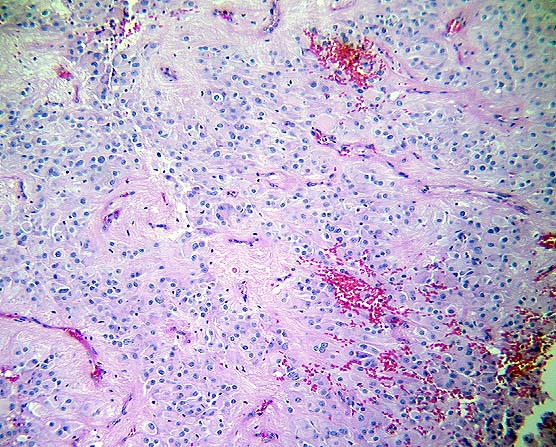
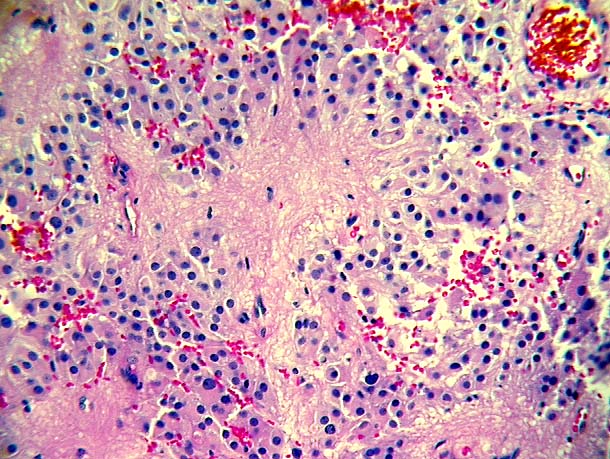
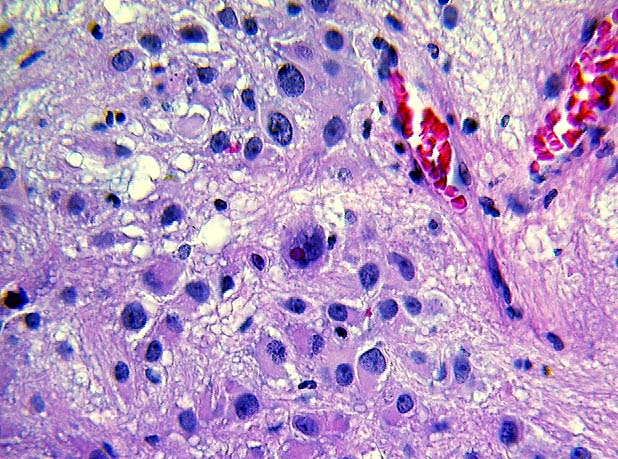
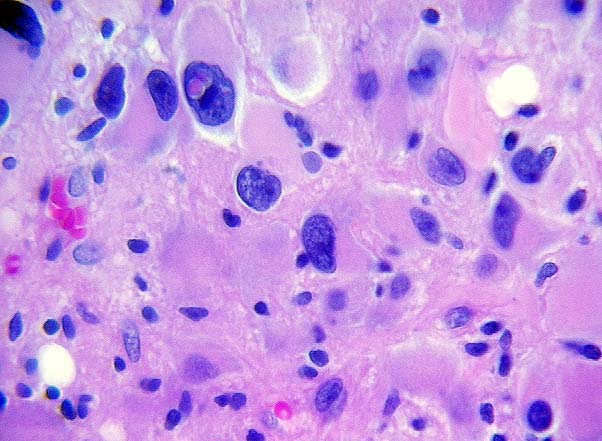
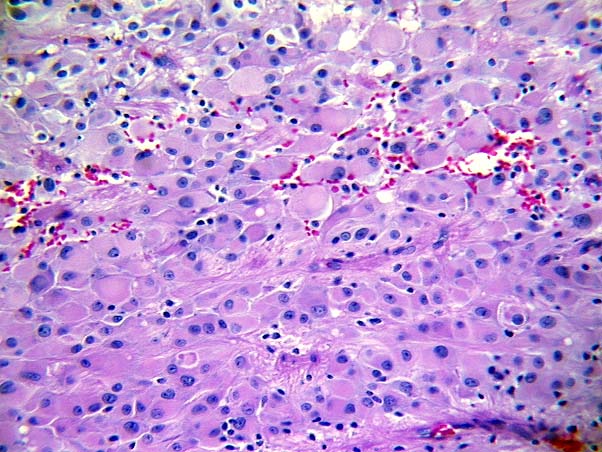
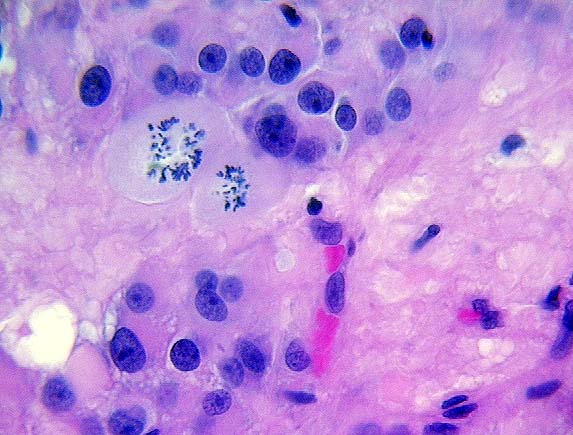
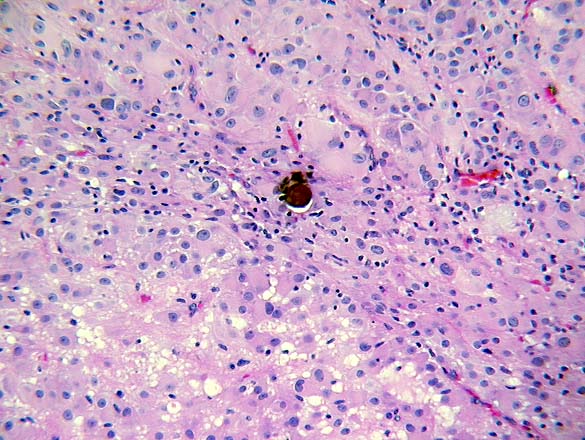
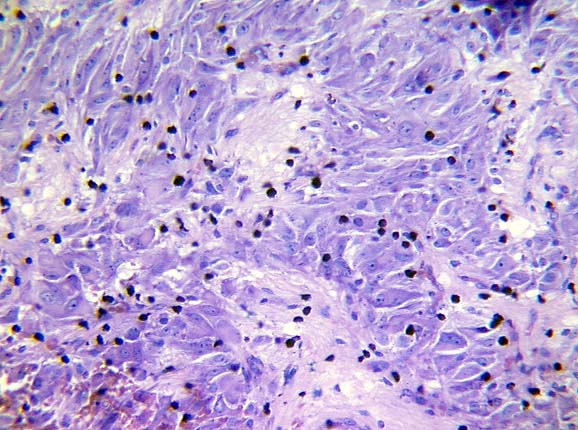
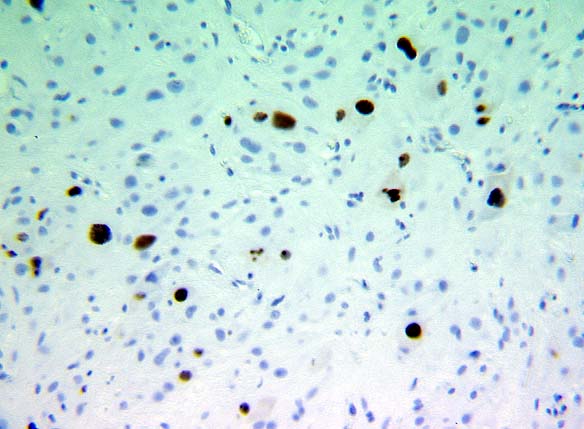
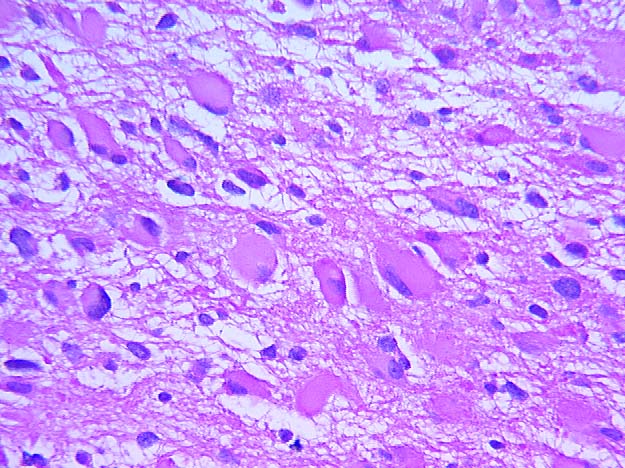
This cellular neoplasm consists of pleomorphic astrocytes in a fibrillar background which focally shows prominent acellular perivascular areas. (Images 03, 04 and 05) The large cells have pleomorphic nuclei with dispersed chromatin and prominent nucleoli, with occasional eosinophilic intranuclear inclusions (Images 06 and 07) and abundant eosinophilic cytoplasm (Image 08). Numerous atypical mitoses are seen, many of which resemble the chromosome spread seen in a karyotype (Image 09). Calcifications are identified (Image 10). Numerous mast cells are highlighted by Giemsa stain (Images 11 and 12). A rare focus of necrosis is identified (Image 13); vascular hyperplasia is not seen. The large tumor cells are focally positive on GFAP immunostaining (Image 14). S100 immunostains many more of the tumor cells (Image 15), although the perivascular acellular areas stain negative for both. Many of the large cells are negative for both GFAP and S100. The large cells are also positive for vimentin and negative for cytokeratins, desmin and EMA. A ki-67 proliferation index is 20.3% (Image 16).
DIFFERENTIAL DIAGNOSIS:
The differential diagnosis of intraventricular tumors include ependymoma, subependymoma, subependymal giant cell astrocytoma (SEGA), choroid plexus tumors, pilocytic astrocytoma, central neurocytoma, pineal and germ cell tumors, papillary craniopharyngioma, colloid cysts and meningioma. Most of these lesions can be diagnosed based on clinical, radiographic and histologic features. A history of tuberous sclerosis (TS) favors SEGA. Although a gemistocytic astrocytoma can resemble SEGA (Image 17) , the astrocytoma typically contains entrapped non-neoplastic neuronal and glial tissue because of its diffusely infiltrative nature, in contrast to the sharply demarcated SEGA. Mast cells and intranuclear pseudo-inclusions are rarely seen in gemistocytic astrocytoma, in contrast to SEGA. Although rare mast cells can be seen in other central nervous system tumors, numerous mast cells are only seen in SEGA. In addition, SEGA only rarely develops into a more malignant glioma, which is a frequent occurrence with gemistocytic astrocytoma. Some SEGAs show numerous mitoses and focal necrosis, but these features do not have a worse prognosis.
Rarely will a SEGA show the mitoses, necrosis and vascular proliferation seen in a glioblastoma multiforme (GBM). SEGA should be distinguished from the giant cell variant of GBM, which is circumscribed grossly, but does not present as an intraventricular tumor.