
FINAL DIAGNOSIS: DISSEMINATED TOXOPLASMOSIS
DISCUSSION
The patient was diagnosed with disseminated toxoplasmosis. The infection was probably a recurrence of a latent infection as serological studies prior to transplantation were negative for IgM and less than 16 for IgG. Involvement of the central nervous system correlated with her mental status changes and seizures and involvement of the lungs correlated with her respiratory failure. Her hospital course typifies toxoplasma infection in bone marrow transplant patients -- fevers of unknown origin, treatment for graft vs host disease, neurological deterioration, and diagnosis made at autopsy.
Toxoplasmosis is caused by Toxoplasma gondii a protozoan parasite with a predilection for involvement of the human brain. The life cycle of T. gondii has both asexual and sexual stages. The sexual stage takes place in the intestines of cats, leading to infective oocytes being excreted in the feces. When cat feces contaminate plant material or water, the oocytes can be ingested by herbivores or omnivores who then become infected. Eating infected animals (it is estimated that 25% of lamb and pork sold at supermarkets contain viable tissue cysts1) is a major source of infections in humans. Cockroaches, snails, slugs, and earthworms can also serve as transports for the oocytes. Once the oocyte enters the host, tachyzoites are released in the small intestine and infect the intestinal epithelium. The tachyzoites then gain access to the circulation and become widely disseminated, with peak blood levels at about day 142. Tachyzoites can parasitize any nucleated cell and can cause considerable tissue damage. Once the immune response has developed, the infection is controlled and tissue cysts are formed. Most tissue cysts eventually disintegrate and become calcified, but some remain viable for weeks to years.
Most human infections occur by one of four routes: (1) consumption of water or plant material contaminated with cat feces, (2) ingestion of undercooked meats, (3) transplacental transmission to a fetus by a mother infected during pregnancy, (4) organ transplantation. The prevalence of T gondii infection ranges from about 20% in the United States to as high as 90% in some regions of France1. Most infections in immunocompetent individuals are asymptomatic. About 10-20% of patients develop symptoms that typically include lymphadenopathy, particularly of the cervical lymph nodes, and often complaints of fever, sore throat, and myalgias.
In cases of maternal to fetal transmission, the risk to the fetus is determined by the gestational age at the time of infection and not by maternal symptoms. Term infants may be able to withstand T gondii infection with the help of maternal immunoglobulins, but premature infants are at particular risk and the tachyzoites are often widely distributed in the fetal tissue. Involvement of the CNS often leads to severe impairments including mental retardation, spasticity, ocular disease, and deafness. For this reason, economic costs associated with toxoplasma infection are the highest of all food-borne pathogens3.
Immunosuppressed patients are particularly susceptible to disseminated infections. Most cases occur in patients with AIDS, bone marrow transplants, or heart transplants. Less frequently, cases have been reported in liver and kidney transplant patients as well as patients with malignancies. Toxoplasmosis in bone marrow and heart transplant patients is further discussed below.
Laboratory diagnosis of Toxoplasmosis
Sabin-Feldman dye test
This test is based on the observation that live tachyzoites stain blue with alkaline methylene blue dye. Live tachyzoites are mixed with different dilutions of the patient's serum and the mixtures are then incubated for an hour, stained with dye, and examined with a microscope. If antibodies to T gondii are present in the patient's serum, they will damage the organisms. The damaged organisms will not take up the dye and appear as pale "ghosts" compared to undamaged organisms. The test requires live tachyzoites and is difficult to perform, so other serological tests are typically used. However, the test is very sensitive and specific and remains the reference method.
Latex agglutination test
In this test, latex particles are coated with inactivated toxoplasma antigens and attached to the bottom of wells in a microtitration tray. The wells are then exposed to different dilutions of the patient's serum. When toxoplasma antibodies are present in the patient's serum, they bind the antigen and form a network of antibody-antigen complexes that agglutinate and precipitate out of solution, appearing as clumps of particulate material in the wells of a microtitration tray. The latex agglutination test is a member of a family of agglutination tests that include such tests as hemagglutination tests, where the antigens are placed on red blood cells instead of latex particles, and the direct agglutination test, where the antigen is fixed on membranes.
Enzyme linked immunoabsorbent assay (ELISA)
In these tests, the patient's antibodies are attached to plastic wells. Toxoplasma antigen is labeled with an enzyme, usually horseradish peroxidase, and added to the wells containing the patient's antibodies. The wells are then rinsed removing all antigen that has not been bound by the patient's antibodies. A substrate for the peroxidase is then added. If the patient has antibodies to toxoplasma, the toxoplasma antigen will have been bound and can be detected by the enzymatic activity. There are many modifications of this basic technique, including methods that use antigens with a fluorescent label.
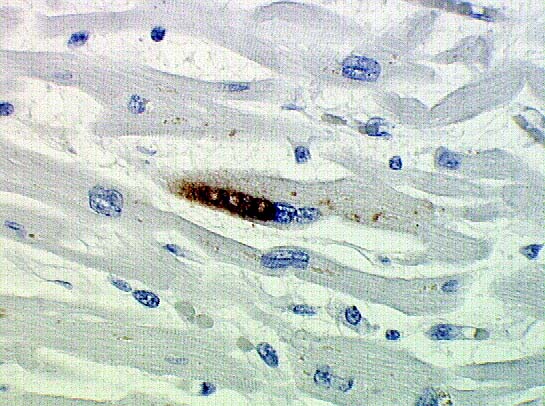
Immunohistochemistry
In a technique very similar to ELISA, antibodies directed against toxoplasma antigens are labeled with immunoperoxidase and applied directly to tissue on a histological slide. (image )
Toxoplasmosis and bone marrow transplantation
Toxoplasmosis is a rare, but serious, complication of bone marrow transplantation, with just over 50 cases described in the literature. Reports in the literature4-8 suggest: 1) most cases of toxoplasmosis are recrudescences of preexisting infections; 2) most occur in patients with allogenic transplants; 3) most occur in the early post transplant interval during the time of maximal immunosuppression; 4) there is an association between the treatment (increased immunosuppression) for graft vs host disease and toxoplasmosis; 5) the diagnosis can be difficult to make as serological studies do not always correlate with clinical disease and lesions amenable to tissue biopsy are frequently not present; thus many cases are not diagnosed until autopsy. In a recent review4, only 4 of 55 patients reported in the literature have survived toxoplasmosis infection.
These general principles are well illustrated by a large series from the University of Washington, Seattle5, that summarized the experience of toxoplasmosis in 3803 consecutive marrow transplant patients, consisting of 3294 allogeneic and 509 autologous transplants, over a 20 year period. None of the autologous bone marrow transplant patients developed toxoplasmosis. An estimated 15% of the patients who received an allogeneic transplant were seropositive for toxoplasma prior to transplantation, indicating past infection, and 2% of these patients (12 cases) developed toxoplasmosis following transplantation. Ten of the 12 cases were diagnosed at autopsy and toxoplasma contributed to the patient's death in 50% of the cases. All of the infections occurred within the first 6 months, during the time of maximal immunosuppression, and 11of the 12 patients had a history of GVHD. A recent study from France has demonstrated the usefulness of prophylaxis with pyrimethamine and sulfadiazine in preventing the development of toxoplasmosis in seropositive patients who undergo allogeneic marrow transplantation10.
Toxoplasmosis and heart transplantation
The incidence of toxoplasmosis in heart transplant recipients is generally higher than that for bone marrow recipients and ranges from 4% to 13% 11,12. In contrast to bone marrow transplant patients, most cases occur as new infections that are acquired from the donor organ. Recrudescence of clinically latent infections occurs much less frequently and the infections are often less serious. Life threatening infections are almost entirely restricted to seronegative patients who receive a heart from a seropositive donor13. Patients can present with a wide variety of symptoms ranging from fevers, to neurological impairment to pneumonitis.
Due to the varied clinical presentation of toxoplasmosis, the diagnosis can be difficult to make. Also, patients can have a delayed seroconversion due to immunosuppresion11. In other patients, serological changes indicating active toxoplasma infection are not always associated with overt clinical disease12. Endomyocardial biopsy can be helpful in making the diagnosis and should be considered especially in culture negative patients with persistent fevers of unknown origin accompanied by neurological symptoms11
REFERENCES
![]() <Contributed by Michael Torbenson, MD, A. Julio Martinez, MD and Larry Nichols, MD
<Contributed by Michael Torbenson, MD, A. Julio Martinez, MD and Larry Nichols, MD