![]() Contributed by Larry Nichols, MD
Contributed by Larry Nichols, MD
![]() Published on line in August 1998
Published on line in August 1998
Disclosure Statement: In accordance with the policies on disclosure of the Accreditation Council for Continuing Medical Education and the Faculty Advisory Committee for Continuing Education in the Health Sciences, University of Pittsburgh, presenters for this program have identified no personal relationships with a health care product company which, in the context of their topics, could be perceived as a real or apparent conflict of interest.
LEARNING OBJECTIVES:
DEGREE OF DIFFICULTY:
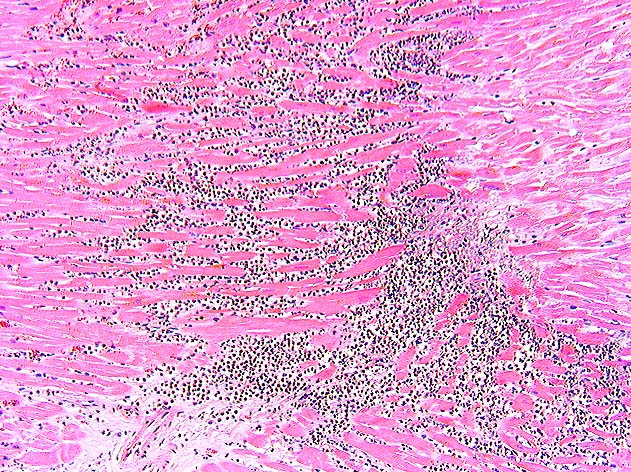
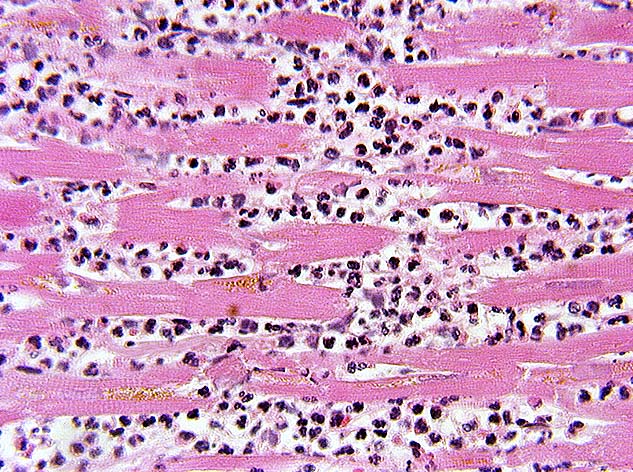
This 49-year-old married white male school teacher was a 2 pack/day smoker with a history of diabetes mellitus, hyperlipidemia and obesity, and a family history of coronary artery disease. He was awakened from his sleep at 03:00 with crushing substernal chest pain which radiated to his left arm and was accompanied by shortness of breath. When paramedics arrived, they found the patient cool, clammy, bradycardic and hypotensive. Intravenous fluids and atropine were given and he was transported to a suburban hospital.
On arrival in the emergency department at the hospital, the patient was in considerable distress. He was still bradycardic. He had no jugular venous distention. He had decreased breath sounds with occasional expiratory wheezes. At 04:01 his white blood cell count was 7,900/cu mm, hematocrit 45.8%, platelets 246,000/cu mm, creatine phosphokinase (CPK) 89 IU/L and troponin-I <0.4 ng/ml. Electrocardiogram showed ST-segment elevation in leads II, III, AVF and V4-V6. Chest x-ray showed borderline cardiomegaly without signs of pulmonary edema.
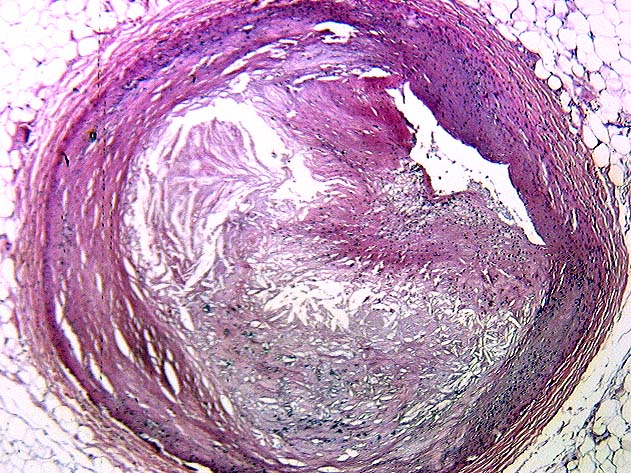
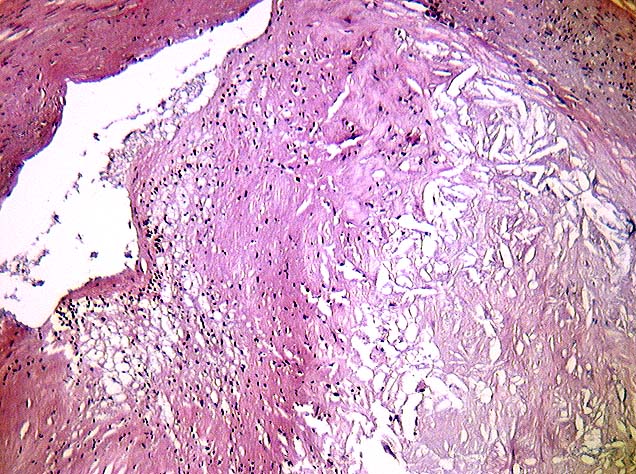
The patient was treated with morphine, atropine and aspirin, but he remained bradycardic and hypotensive. He had decreasing pulse oximeter blood oxygen saturation despite supplemental oxygen and he became cyanotic. He was intubated. A transcutaneous pacemaker was placed. A dopamine drip was started, resulting in an increase in the patient's blood pressure. He was started on heparin and emergency cardiac catheterization showed non-critical disease of the left anterior descending and left circumflex arteries but a dominant right coronary artery which was totally occluded proximally. Percutaneous transluminal coronary angioplasty (PTCA) was attempted but failed to re-open the right coronary artery. An intra-aortic balloon pump was placed and the patient was transferred via helicopter to the university hospital. At the university hospital, his total CPK rose to 4422 IU/L (MB isoenzyme 223.8 ng/ml, relative index 5.1). The evolving clinical data made it clear that his prognosis was extremely grim. He was given comfort measures and he died peacefully.