
![]() Contributed by Jeff Kleinberger, MD, PhD and Gabriel Sica, MD, PhD
Contributed by Jeff Kleinberger, MD, PhD and Gabriel Sica, MD, PhD
CLINICAL HISTORY
A man in his 60's with a history of metastatic lung adenocarcinoma presents with progression of disease identified by positron emission tomography (PET) scan. He was initially diagnosed with lung cancer 4 years prior, when a 5.0 cm left infrahilar mass and left hilar lymphadenopathy was identified. At that time, cytologic evaluation of an endobronchial ultrasound-guided fine needle aspiration of his subcarinal lymph node demonstrated metastatic lung adenocarcinoma (Figure 1). Next-generation sequencing of the tumor using an oncologic hotspot panel identified an EGFR exon 19 deletion (p.E746_A750del), but no other mutations. Fluorescence in-situ hybridization studies (FISH) did not identify ALK rearrangement, ROS1 translocation, RET translocation, or MET amplification. Immunohistochemistry showed PD-L1 was expressed on 1% of the malignant cells. The tumor was classified as unresectable stage IIIC lung adenocarcinoma, cT3 N3.
Figure 1: High Magnification Images of Endobronchial Ultrasound Guided Fine-Needle Aspiration of Subcarinal Lymph Node, Initial Diagnosis
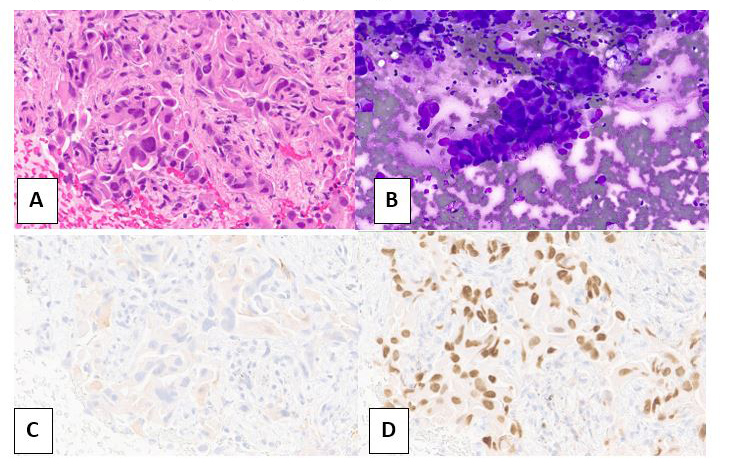
A: Hematoxylin and eosin stain of cell block material, B: Diff-Quik stain of cytologic specimen,
C: Synaptophysin immunohistochemical stain, D: TTF-1 immunohistochemical stain
The patient was treated with osimertinib and had a good initial response that was followed by interval increase in the size of the primary tumor and possible metastases to the bone. Osimertinib was paused and replaced with a carboplatin/etoposide regimen and radiation therapy, which resulted in a good initial response. A month later he had a cerebrovascular accident, and during work up, several brain metastases were discovered. Subsequent PET scan identified new metastases in the right adrenal gland and left iliac bone, leading to his current presentation.
Biopsy of the FDG-avid right adrenal gland mass was performed. Figure 2 shows the adrenal gland mass biopsy and immunohistochemical stain work up.
Figure 2: High Magnification Images of Ultrasound Guided Biopsy and Touch Prep of FDG-Avid Adrenal Mass, current specimen
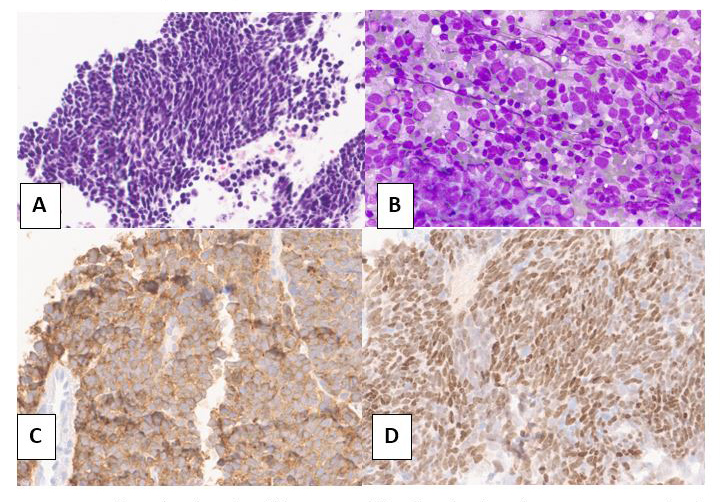
A: Hematoxylin and eosin stain of biopsy, B: Diff-Quik stain of touch prep,
C: Synaptophysin immunohistochemical stain, D: TTF-1 immunohistochemical stain
Repeat next generation sequencing using the same oncologic hotspot panel on the adrenal mass identified the same EGFR exon 19 deletion (p.E746_A750del), but also mutations in TP53 (p.R337C) and RB1 (frameshift mutation).
What is your diagnosis?