FINAL DIAGNOSIS
Mucinous cystadenocarcinoma (MCA) of the breast.
DISCUSSION
Mucinous cystadenocarcinoma of the breast (MCA) was first described by Koenig and Tavassoli in 1998 as a tumor composed of variably sized cystic spaces lined by neoplastic mucinous cells with bland, basally placed nuclei forming epithelial tufts and papillae. The interpretation of this tumor as an invasive carcinoma is confirmed by the absence of a myoepithelial cell layer on immunohistochemical staining. The 21 reported cases of MCA have shown varying degrees of cytologic atypia as well as varying degrees of mucin depletion and cytoplasmic eosinophilia. This characteristic tumor morphology mimics metastatic mucinous carcinomas of the ovary, pancreas and GI tract; thus, an IHC panel should be ordered including CK7+, CK20-, CDX2-, PAX8-, WT1-, MAMG+, GCDFP15+, GATA3+, ER-, PR-, and Her2-. The breast markers are highly specific but not sensitive; therefore, positive stains are contributory whereas negative stains are noncontributory. This entity should also not be confused with invasive mucinous carcinomas or signet ring cell carcinomas of the breast.
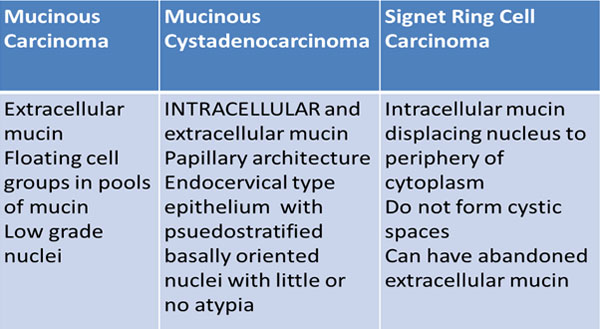
Invasive mucinous carcinoma contains extracellular mucin and signet ring cell carcinoma contains intracellular mucin, but MCA can be distinguished from these entities as it has intra- and extracellular mucin, a characteristic tufting pattern, and it lacks the displaced nuclear cytology of signet ring cells.
The reported cases of MCA have shown that this entity does not behave clinically as other ER-/PR-/HER2- tumors with a high KI67 index (5-70%). The likelihood of lymph node metastasis does not correlate with pathologic staging (15%), and no recurrences or distant metastases have been reported so far. Thus, MCA is considered to be an indolent behaving tumor requiring complete excision with sentinel lymph node dissection. The role of chemotherapy and radiation in these tumors is unknown.
For pathologic staging purposes, the entire tumor should be measured as the invasive tumor component. MCA type ductal carcinoma in situ has been reported, but if myoepithelial markers are negative, the invasive component will account for the greatest dimension of the mass such as in this case.
REFERENCES
![]() Contributed by: Dorian Infantino, MD
Contributed by: Dorian Infantino, MD