

FINAL DIAGNOSIS
DISCUSSION
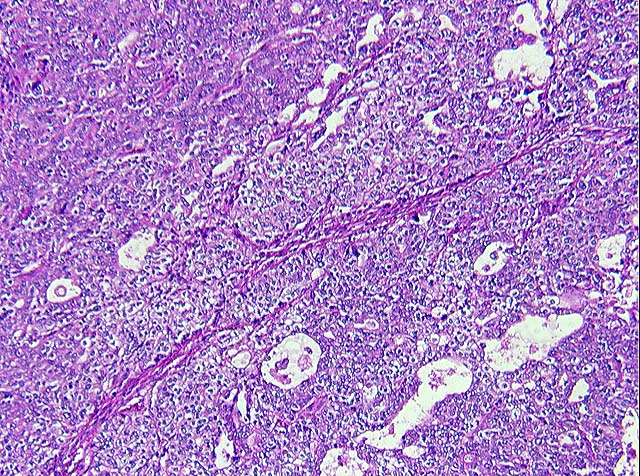
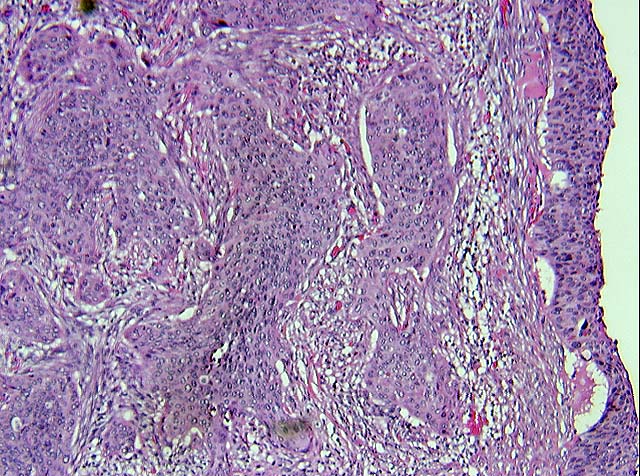
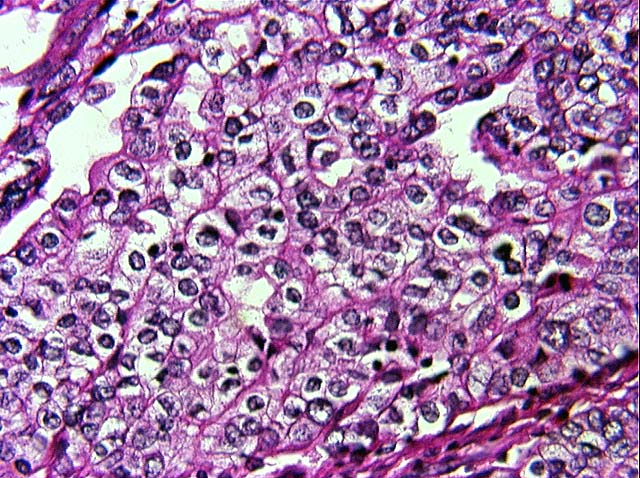
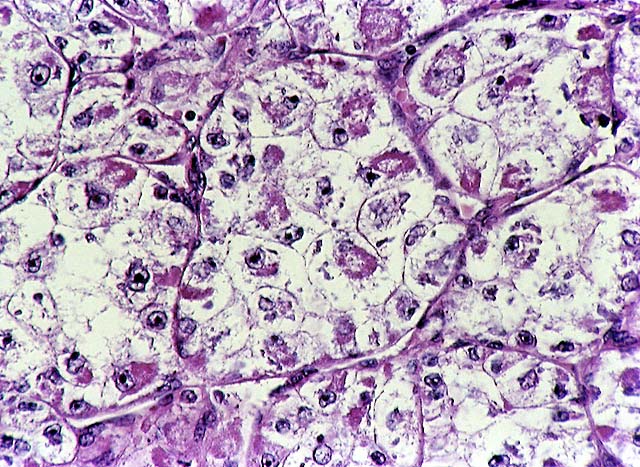
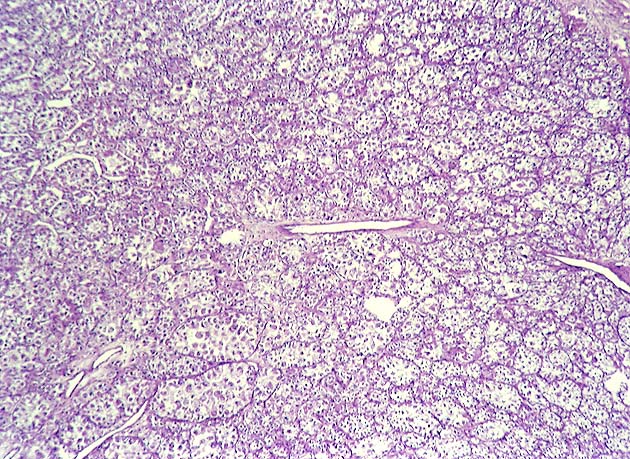
Glassy cell carcinoma of the cervix is a form of poorly differentiated adenosquamous carcinoma arising from the subcylindrical reserve cells. It comprises less than 1%of all cervical carcinomas. It typically affects younger patients compared to other invasive cervical carcinomas, with a peak incidence in the 3rd to 4th decade. Some studies have noted an association with pregnancy. These tumors present as rapidly growing bulky exophytic masses, or with a barrel shaped cervix. Histologically, they are characterized by sheets of large polygonal cells with finely granular ground glass type cytoplasm. These cells have distinct cell borders, vesicular nuclei with prominent nucleoli. The majority of the tumor cells lack intracellular bridges, dyskeratosis and intracellular glycogen. However, focal abortive keratin production, squamous or glandular differentiation may be present. There may be focal clear cell differentiation. Mitotic figures are frequently seen. The stroma is heavily infiltrated by lymphocytes, plasma cells and eosinophils. Glassy cells can show focal mucin and CEA positivity. Ultrastuctural findings show evidence of both squamous and glandular differentiation, including well developed desmosomal complexes and microvilli. The ultrastructural correlate of the glassy cytoplasm is unclear. DNA of human papilloma virus types 18 and 16 have been detected in the tumor cells of glassy cell carcinoma.
The differential diagnosis is with other poorly differentiated neoplasms involving the cervix including; large cell non keratinizing squamous cell carcinoma, (Image 13, Image 14)poorly differentiated adenocarcinoma (Image 11, Image 12), clear cell carcinoma (Image 15) and clear cell sarcoma (alveolar soft part sarcoma of the female genital tract). Although glassy cell carcinomas may have focal squamous or adenocarcinmatous differentiation, a prominent component is not usually seen. Although these tumors may show a plasmacytic and eosinophilic infiltrate, the glassy cell carcinoma often has an extensive eosinophilic infiltrate which is characteristic. Clear cell carcinomas contain abundant intracellular glycogen in contrast to the relative absence of it in glassy cell (Image 15) carcinoma. Alveolar soft part sarcoma is a well circumscribed tumor with an alveolar pattern and PAS positive crystals within the cytoplasm. (Image 16 & Image 17)
The clinical course is that of an aggressive tumor with a tendency to metastasize early. Patients who present with smaller, exophytic masses tend to be diagnosed earlier, and when treated aggressively, fare better than those patients who present with endophytic tumors. Treatment is aggressive with radical hysterectomy and adjuvant irradiation. The biologic behavior of glassy cell carcinoma is similar to the other poorly differentiated carcinomas mentioned above, but it distinguishes itself by affecting younger patients, making early recognition extremely important.
Glassy cell carcinomas have also been reported in the endometrium and colon.
REFERENCES
![]() Contributed by Peter Christakos, MD and Manju E. Nath MD.
Contributed by Peter Christakos, MD and Manju E. Nath MD.