DIAGNOSIS: CONSISTENT WITH CNS LYME DISEASE
Contributor's Note:
Lyme disease develops following infection with the tick-borne spirochete, Borrelia burgdorferi. The disease course proceeds through three stages.
Adults are more likely to manifest symptoms of neuroberreliosis than are children. These symptoms can include peripheral nerve parasthesias, a Guillain-Barre-like syndrome and Bannwarth's syndrome (lymphocytic meningoradiculitis).(2) A study by Hansen et al. showed that patients with neuroborreliosis demonstrate a blood brain barrier disturbance with 62 % showing an elevated albumin ratio and 60 % revealing an increased IgG index, indicative of intrathecal IgG synthesis. In addition, 51 % of patients exhibited oligoclonal IgG bands and these bands were more likely to be present with a longer time since onset of neurologic symptoms. (3)
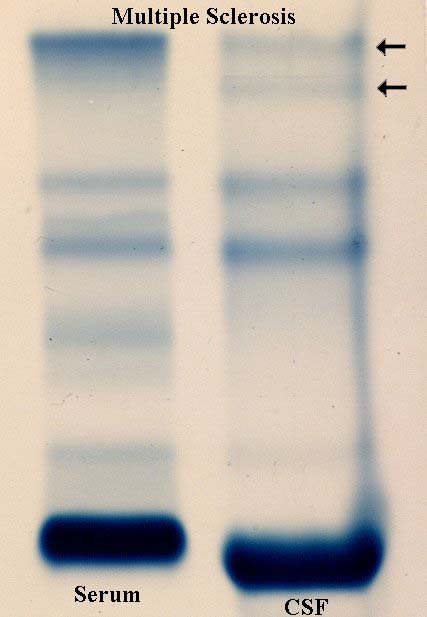
Immune complexes can be recognized by their distinctive staining pattern on zone electrophoresis. B cells in the CNS may give rise to a clonal proliferation of immunoglobulins within the CSF which will appear as a distinct, restricted band in the gamma region of the zone electrophoresis gel. Immune complexes occur when the antibody binds an antigen which results in a slight shift in antibody migration on the gel resulting in blurring or "bridging" of the band (4,5). As can be seen in the CSF protein electrophoresis pattern, there are immune complexes present in this patient's CSF. The immune complexes are indicated by arrows.
Neuroimaging studies may demonstrate discrete, hyperintense, deep white matter of periventricular lesion best visualized on proton density and T2 weighted images.
In this patient, a possible diagnosis of multiple sclerosis (MS) must also be considered based on the neurologic, immunologic and radiologic presentation. However, the increased permeability of the blood brain barrier and the oligoclonal band bridging (immune complex formation) favor an infectious process over a demyelinating process.
REFERENCES:
{kind=link}
{kind=link}