

The clinicopathologic differential diagnosis includes predominantly the microscopic form of polyarteritis nodosa (polyarteritis nodosa with glomerular involvement) and Wegener's granulomatosis. The presence of extrarenal (pulmonary) involvement and granulomatous vasculitis favors Wegener's granulomatosus, despite the absence of upper respiratory tract involvement and p-ANCA rather than c-ANCA seropositivity. The acute tubular injury which was suspected clinically appears to be secondary to the glomerular disease. Given the predominantly active inflammatory changes with absence of chronicity changes, aggressive medical therapy including cytoxan was recommended.
Contributor's Note:
Crescentic glomerulonephritis or rapidly progressive glomerulonephritis (RPGN) is a term given to a diverse group of diseases which all have cresents present within the glomerular tuft (Table 1). These include primary or renal limited (so-called idiopathic) crescentic glomerulonephritis, anti-glomerular basment membrane(anti-GBM) antibody diseases, and systemic disorders. Considered within the entire clinical spectrum of renal disease, RPGN produces the most rapidly progressive and destructive of glomerular diseases which in the most severe forms proceeds inexorably to renal failure if not treated aggressively and early. (Table 2). Fortunately, RPGN accounts for only 2 to 7% of renal biopsies, with a disproportionately large percentage of these patients progressing to end stage renal disease. proportion of all patients with end-stage renal disease.
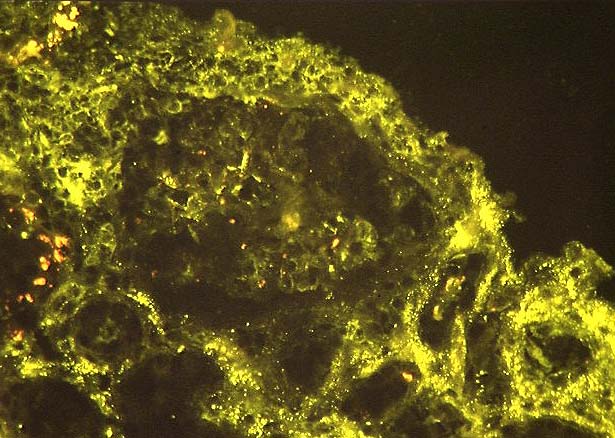
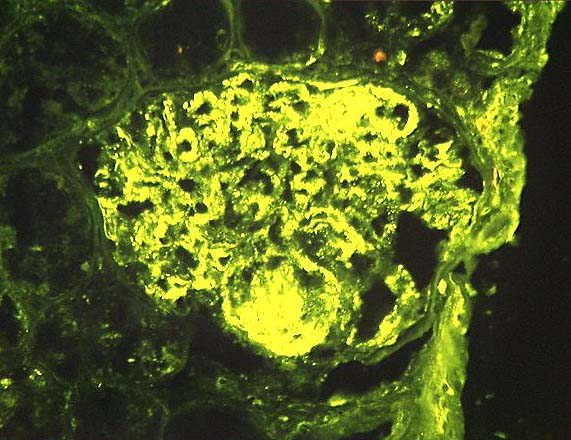
RPGN is categorized based on the biopsy immunofluorescence pattern into three groups: RPGN Type I (20%), RPGN Type II (40%), and RPGN Type III (40%) (Table 3). RPGN types I and II have greater than 2+ (on a 4+ scale) immunofluorescence staining intensity with linear (Figure 1) and granular (Figure 2) staining patterns, respectively. RPGN Type III or pauci-immune type (Figure 3) has weak or no demonstrable immunoglobulin / complement deposition, corresponding to an immunofluorescence staining intensity of < 2+.
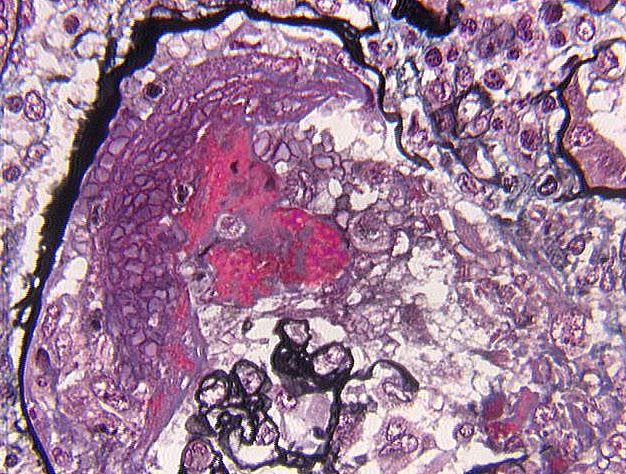
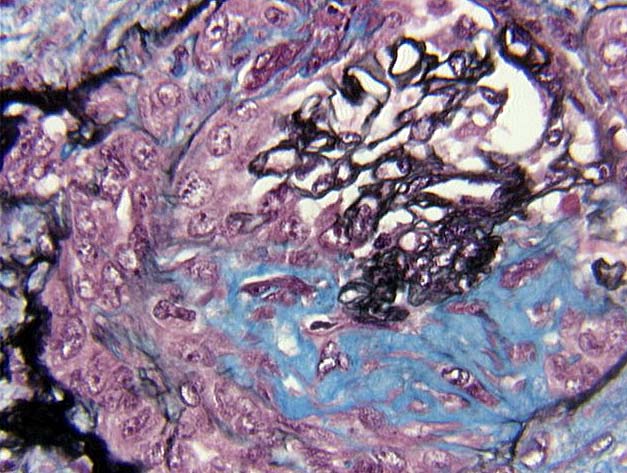
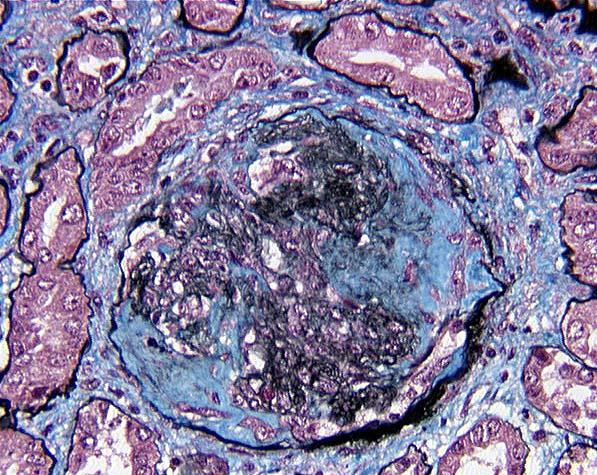
Light microscopic examination typically shows at least 30% of the glomeruli involved by crescents. Overall the number of crescents is about the same for all three forms resulting in an RPGN clinical picture, which typically show 50-100% involvement by crescents. Anti-GBM disease and pauci-immune forms of necrotizing glomerulonephritis tend to be associated with a higher percentage of crescents compared to immune complex diseases, and are therefore more likely to produce an RPGN clinical presentation. The crescents may be seen at various stages of evolution from early basement membrane breaks with leakage of blood in Bowman's space (Figure 4) to cellular crescent formation (Figure 5) to fibrocellular cresent formation (Figure 6) and finally the fibrous crescent (Figure 7) in which collagen has filled Bowman's space.
Light microscopy can provide useful information to help distinguish which subclass (RPGN I, II, III) of crescentic glomulonephritis is present. RPGN type II have more segmental hypercellularity than types I and III. Necrotizing changes of glomerular tufts are more common in RPGN types I and III. In particular, comparing RPGN Type I to RPGN type III, the pauci-immune disease is more often associated with necrotizing arteritis while the anti-GBM disease is usually associated with a capillaritis.
| Disease Category (Most to Least Severe) | RPGN (Most Severe) | Nephritic syndrome (e.g. post-infectious GN) | Nephrotic syndrome(e.g. Minimal change disease) | Chronic progressive glomerulopathy (e.g. Diabetes nephropathy) | Asymptomatic (e.g. Thin basement membrane disease) (Least Severe) |
|---|---|---|---|---|---|
| Clinical Signs/Symptoms | Acute renal failure plus nephritic syndrome | Hypertension, RBC casts, Hematuria, Azotemia | Greater than 3.5 gm of protein in 24 hr urine | Insidious progressive loss of renal function | Microscopic hematuria |
Table 3 - Three Types of RPGN Based on Immunofluorescence Pattern
| Type | Pathogenesis | Disease(s) | Pattern | Strength |
|---|---|---|---|---|
| I | Anti-GBM | Goodpasture's disease | Linear IgG, Weak linear C3 | greater than 2+ |
| II | Immune complex | SLE, IgA nephropathy | Granular Ig and C3 capillary loop/mesangium | greater than 2+ |
| III | Pauci-immune or Unknown | Wegener's Syndrome | Weak/Absent staining | less than 2+ |
References
Couser WG. Rapidly progressive glomerulonephritis: classification, pathogenetic mechanisms, and therapy. American Journal of Kidney Diseases 11(6); 449-464: 1988.
Couser WG. Pathogenesis of glomerulonephritis. Kidney International 44 Suppl. 42; S19-S26: 1993.
Weiss MA, Crissman JD. Renal biopsy findings in Wegener's granulomatosis: segmental necrotizing glomerulonephritis with glomerular thrombosis. Human Pathology 15(10): 1984.
Pathology of the Kidney. Heptinstall RH, Little Brown and Company, Boston, MA, 1992.
![]() Contributed by Curtis S. Goldblatt, M.D. and Sheldon Bastacky, M.D.
Contributed by Curtis S. Goldblatt, M.D. and Sheldon Bastacky, M.D.