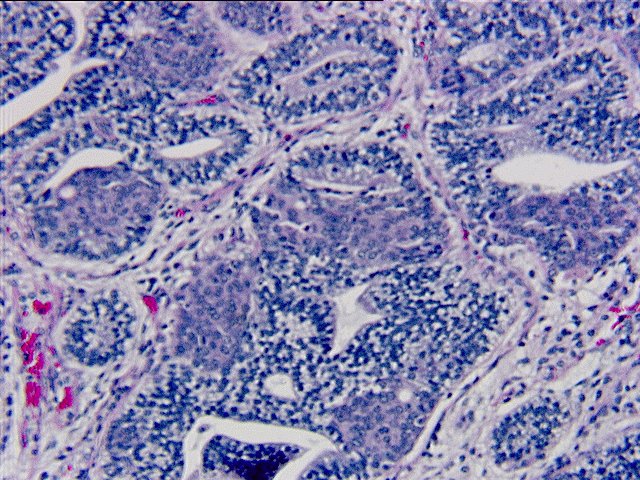

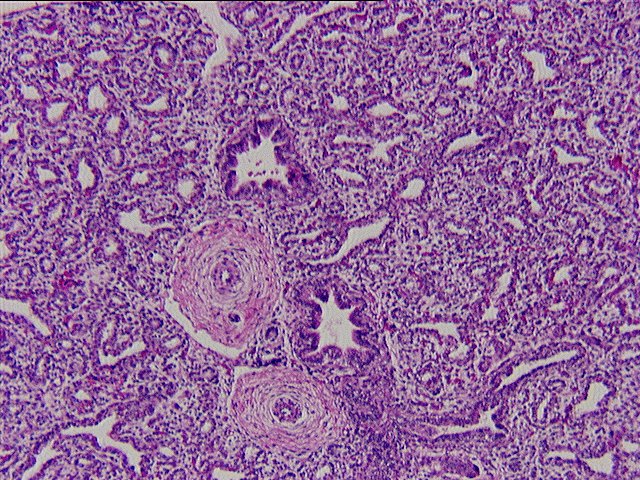
The infiltrating adenocarcinoma has a distinctive histologic appearance. It forms glands, with a vague papillary architecture, comprised of columnar cells with nuclear stratification and extensive cytoplasmic clearing. Intraluminal mucin is identified however both diastase predigested PAS stains and Mucicarmine stains fail to show significant cytoplasmic mucin. This overall histologic appearance corresponds to that described with fetal type adenocarcinomas, or what has been previously classified as monophasic pulmonary blastoma. Another interesting feature of this tumor is it's proximity to a large subpleural pulmonary scar. This scar is associated with thrombosis of numerous arteries and veins, and strongly suggests that it derived from a previous pulmonary infarct.
CONTRIBUTOR'S NOTE :
Well-differentiated fetal type adenocarcinomas are one of three morphologic varieties of pulmonary blastomas. Pulmonary blastomas are rare malignancies, comprising 0.5% of all primary lung malignancies. These lesions are composed of immature epithelial and/or mesenchymal components and a resemblance to fetal lung has been noted. Classic biphasic pulmonary blastomas and pleuropulmonary blastomas represent the two other morphologic categories of pulmonary blastomas. Each morphologic category has its own classic patient population, presentation, and histologic appearance.
The well-differentiated fetal type adenocarcinoma, the category of pulmonary blastoma noted in this case, has a mean age of onset of 33 years and equal sex distribution. A history of smoking is reported in approximately 80% of cases. Patients are asymptomatic in 60% of cases and pleural effusions are rare. Grossly, these lesions are usually solitary, peripheral, well-circumscribed, and variegated in color. The histologic appearance of well-differentiated fetal type adenocarcinomas is as described in this case. However, the histologic characteristic of morular metaplasia, that is often noted in well-differentiated fetal type adenocarcinomas, is absent in this case. Optically clear nuclei may be seen within the areas of morular metaplasia. Immunohistochemistry typically demonstrates cytokeratin, epithlial membrane antigen, and carcinoembryonic antigen positivity. Interestingly, focal chromogranin and neuron specific enolase positivity may be demonstrated.
Differentiation of well-differentiated fetal type adenocarcinoma from a typical primary lung adenocarcinoma includes presence of the classic morphology of the well-differentiated fetal type adenocarcinoma with tall columnar cells, supra and subnuclear vacuolization, morular metaplasia, and optically clear nuclei. Also, demonstration of abundant intracytoplasmic glycogen is helpful in the distinction. Prognostic factors which are related to decreased survival in well-differentiated fetal type adenocarcinomas include, as one might expect, thoracic lymphadenopathy, recurrence, metastasis at presentation, and pathologic stage greater than stage I. The prognosis of well- differentiated fetal type adenocarcinoma may be better than that of a typical lung adenocarcinoma. According to Koss et. al., 81% of patients with well-differentiated fetal type adenocarcinoma in their study group were alive with no tumor at a mean follow up of 97 months.
In summary, well-differentiated fetal type adenocarcinoma is one morphologic variety of pulmonary blastoma. Differentiation from a typical primary lung adenocarcinoma, by recognizing the classic histologic appearance and the use of histochemical stains, is important due to the potential of improved prognosis in the case of the well-differentiated fetal type adenocarcinoma.
REFERENCES
1. Koss MN, Hochholzer L, Oleary T. Pulmonary Blastomas. Cancer 1991;67:2368-81.
2. Nakatani Y, Dickersin GR, Mark EJ. Pulmonary Endodermal Tumor Resembling Fetal Lung.
Human Pathol 1990;21:1097-1107.
3. Yousem SA, Wick MR, Randhawa P, Manivel JC. Pulmonary Blastoma: an
immunohistochemical analysis with fetal lung in its pseudoglandular stage. Am J Clin
Pathol 1990;93:167-175.
![]() Contributed by Valerie Holst, M.D.and Sam Yousem, M.D.
Contributed by Valerie Holst, M.D.and Sam Yousem, M.D.
{kind=link}
{kind=link}
{kind=link}