Profiles of Total CK, CK-MB and Troponin I in Acute Myocardial Infarction (AMI)
DISCUSSION
The diagnosis of AMI is usually predicated on the WHO criteria of chest pain, ECG changes, and increases in biochemical markers of myocardial injury. Unfortunately, about half of the patients with "typical" symptoms do not have AMI. The diagnosis of AMI is particularly difficult in the elderly, where relatively minor symptoms may reflect acute ischemia. The ECG is specific for AMI, but lacks sensitivity. It also provides additional information regarding localization and the extent of the injury. Sometimes, it is not easy to distinguish remote injury from a more recent one. In contrast, biochemical markers have excellent sensitivity for diagnosing AMI. By combining the most sensitive and the most specific tests, diagnostic accuracy can be enhanced.
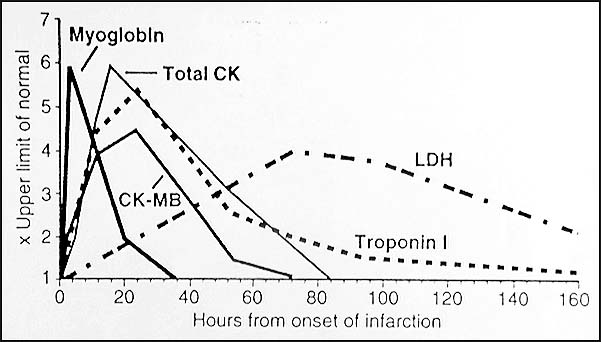
 The patient presented in the first case developed ECG changes that were initially interpreted as nonspecific, until elevated cardiac enzymes were found. At that time, he was asymptomatic, and remained that way during his hospital course. He experienced only intraoperative and brief postoperative hypotension. Nevertheless, his laboratory results indicated the presence of "silent" myocardial infarction. The ECG, is a cornerstone in the diagnosis of acute and chronic ischemic heart disease, when it fails to show conclusive evidence of infarction, the crucial step in ruling in/out the diagnosis of AMI is the measurement of myocardial enzymes in the serum. The rate of release of specific proteins differs depending on their intracellular location, molecular weight, and the local blood and lymphatic flow. The temporal pattern of marker protein release is of diagnostic importance (Graph 1).
The patient presented in the first case developed ECG changes that were initially interpreted as nonspecific, until elevated cardiac enzymes were found. At that time, he was asymptomatic, and remained that way during his hospital course. He experienced only intraoperative and brief postoperative hypotension. Nevertheless, his laboratory results indicated the presence of "silent" myocardial infarction. The ECG, is a cornerstone in the diagnosis of acute and chronic ischemic heart disease, when it fails to show conclusive evidence of infarction, the crucial step in ruling in/out the diagnosis of AMI is the measurement of myocardial enzymes in the serum. The rate of release of specific proteins differs depending on their intracellular location, molecular weight, and the local blood and lymphatic flow. The temporal pattern of marker protein release is of diagnostic importance (Graph 1).
Ruling out AMI requires a test with high diagnostic sensitivity, whereas ruling in AMI requires a test with high diagnostic specificity. These diagnostic strategies often require different decision thresholds for different biochemical markers. The ideal marker of myocardial injury would provide early diagnosis, assessment of the success of reperfusion after thrombolytic therapy, detection of re-occlusion and re-infarctions, determination of infarct size, and detection of perioperative MI during cardiac or noncardiac surgery. Acceptable biochemical markers of ischemic heart disease are now considered to include myoglobin, CK-MB, total CK, and cardiac troponins T and I. Enzyme CK has three isoforms composed of two chains (M and B chains), MM, MB and BB. The MB fraction is found predominantly in cardiac muscle. It is important to show both a rise in the serum concentration of CK-MB, and a rise in the ratio of CK-MB to total CK to diagnose MI. Furthermore, it is important to obtain serial samples for CK-MB and total CK from a patient with suspected MI to demonstrate a rise or fall in isoenzyme concentration. Typically, CK-MB begins to rise 4-8 hours after the MI, peaks within the first 24 hours, and can be used to establish the diagnosis of the MI. The CK-MB returns to normal range after 48-72 hours. Case 2 illustrates the use of this marker to confirm clinical diagnosis, as mentioned above. It can also be used for follow up, as an additional tool in evaluation of cardiac patients.
Troponin I is the subunit of the troponin complex that binds actin and inhibits actomyosin ATPase activity in the absence of calcium (http://sbweb.med.harvard. edu/~bcmp/sm_gergely.gif). Three isoforms of troponin I have been described, one cardiac (cTnI), and two skeletal muscle (slow twitch, sTnI, and fast twitch, fTnI) . Each of the three TnI isoforms is encoded by different genes located on different chromosomes. cTnI gene locus maps to 19q13.4. cTnI (MW 24 kDa) and is a unique protein that is different form either fTnI or sTnI (MW 19.8 kDa) because of the presence of additional 31 amino acids at the N-terminal region. Unlike CK-MB, cardiac troponins are not found in serum from healthy people. These facts make cTnI an excellent biochemical marker for detection of myocardial injury.
cTnI has been shown to be a very sensitive and specific marker for acute MI. It can be detected within 4-8 hrs after the onset of symptoms. Therefore, cTnI does not provide an earlier detection of AMI than CK-MB. cTnI peaks between 14-36 hrs after onset of AMI and remains elevated for 5-7 days after AMI. Due to long duration of increase of cTnI following onset of chest pain, it could replace LD-2 isoenzyme for the detection of late presenting AMI patients. Additionally, recent studies demonstrate that cTnI is more sensitive than the LD1/LD2 ratio. The time course of cTnI is affected by re-perfusion, which leads to a more rapid increase, a higher rate of increase, and earlier peak values. This dependence of troponin time course on reperfusion can be used for monitoring the effectiveness of reperfusion therapy. cTnI seems to be of value in determining whether elevations of CK-MB are indicative of myocardial injury or represent skeletal muscle damage in patients with neuromuscular disorders. Troponin I in patients with coronary syndromes permits the early identification of patients with increased risk of MI and cardiac death. Many studies have determined the importance of increased cTnI for the detection of cardiac injury in several patient groups that have often shown falsely increased CK-MB. These groups have included patients with chest and muscle trauma, with cocaine-associated chest pain, in the critically ill, intensive care patients, and in patients with renal disease. cTnI has proved to be a diagnostic and prognostic marker for myocardial damage with high diagnostic sensitivity and specificity. It is a powerful tool for risk stratification and management of patients with unstable angina, even in the presence of normal CK and CK-MB values. Recently, some newer biochemical markers of myocardial injury are being used. One of earliest markers is myoglobin, which is very sensitive but, in certain clinical settings, lacks specificity. An example of that is Case 1, where muscle (not just myocardial) injury would case a myoglobin level increase that would be difficult to interpret. Additional difficulties are present in patients with renal failure, where use of serum myoglobin/carbonic anhydrase III has been advocated by some authors, as myoglobin itself is not reliable enough. Its diagnostic value is primarily due to its early appearance.
These 2 cases demonstrates that cardiac enzyme measurements are a necessary part of the full evaluation of patients with suspected cardiac events, and that such test results can be used for diagnostic purposes as well as for follow up and confirmation of clinical diagnosis.
REFERENCES:
- Henry JB. Clinical diagnosis and management by laboratory methods. 19th edition, 1996;88-89.
- Moqensen J, Kruse TA, Borglum AD. Assignment of the human cTnI gene (TNNI3) to chromosome 19q13.4 by radiation hybrid mapping. Cytogenet Cell Genet 1997;79:272.
- Adams JE, Schectman KB, Landt Y, Ladenson JH, Jaffe AS. Comparable detection of acute myocardial infarction by creatine kinase MB isoenzyme and cardiac troponin I. Clin Chem 1994;40:1291.
- Jaffe AS, Landt Y, Parvin CA, Abendschein D, Geltman EM, Ladenson JH. Comparative sensitivity of cardiac troponin I and lactate dehydrogenase isoenzymes for diagnosing acute myocardial infarction. Clin Chem 1996;42:1770.
- Fiocchi R, Vernocchi A, Gariboldi F, Senni M, Mamprin F, Gamba A. Troponin I as a specific marker for heart damage after heart transplantation in a patient with Becker type muscular dystrophy. J Heart Lung Transplant 1997;16:969.
- Stanton E, Jackowski G, Worron I, Lawrence M, Tanser P, Luxton G, Bonnell R, Gawas Y. Biochemical differentiation between the different classes of unstable angina. J Heart Failure 1995;2:A387.
- Luscher Ms, Thygesen K, Ravkilde J, Heickendorff L. Applicability of cardiac troponin T and I for eary risk stratification in unstable coronary artery disease. TRIM study group. Thrombin inhibition in myocardial ischemia. Circulation 1997;96:2578.
- Green GB, Li DJ, Bessman ES, Cox JL, Kelen GD, Chan DW. The prognostic significance of troponin I and troponin T. Acad Emerg Med 1998;5:758.
- Hamm CW, Goldmann BU, Heeschen C, Kreymann G, Berger J, Meinertz T. Emergency room triage of patients with acute chest pain by means of rapid testing for cardiac troponin T or troponin I. N Engl J Med 1997;337:1648.
- McLaurin M, Apple FS, Henry TD, Sharkey SW. Cardiac troponin I and T concentrations in patients with cocaine associated chest pain. Ann Clin Biochem 1996;33:1.
- Vuori J, Huttunen K, Vuotikka P, Vaananen HK. The use of myoglobin/carbonic anhydrase III ratio as a marker for myocardial damage in patients with renal failure. Clin Chim Acta 1997;265:33-40.
 Contributed by Sanja Dacic, MD, PhD and Mohamed A Virji, MD, PhD
Contributed by Sanja Dacic, MD, PhD and Mohamed A Virji, MD, PhD




 The patient presented in the first case developed ECG changes that were initially interpreted as nonspecific, until elevated cardiac enzymes were found. At that time, he was asymptomatic, and remained that way during his hospital course. He experienced only intraoperative and brief postoperative hypotension. Nevertheless, his laboratory results indicated the presence of "silent" myocardial infarction. The ECG, is a cornerstone in the diagnosis of acute and chronic ischemic heart disease, when it fails to show conclusive evidence of infarction, the crucial step in ruling in/out the diagnosis of AMI is the measurement of myocardial enzymes in the serum. The rate of release of specific proteins differs depending on their intracellular location, molecular weight, and the local blood and lymphatic flow. The temporal pattern of marker protein release is of diagnostic importance (Graph 1).
The patient presented in the first case developed ECG changes that were initially interpreted as nonspecific, until elevated cardiac enzymes were found. At that time, he was asymptomatic, and remained that way during his hospital course. He experienced only intraoperative and brief postoperative hypotension. Nevertheless, his laboratory results indicated the presence of "silent" myocardial infarction. The ECG, is a cornerstone in the diagnosis of acute and chronic ischemic heart disease, when it fails to show conclusive evidence of infarction, the crucial step in ruling in/out the diagnosis of AMI is the measurement of myocardial enzymes in the serum. The rate of release of specific proteins differs depending on their intracellular location, molecular weight, and the local blood and lymphatic flow. The temporal pattern of marker protein release is of diagnostic importance (Graph 1).