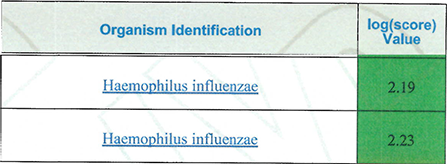
Figure 3. MALDI-TOF results DISCUSSION
FINAL DIAGNOSIS
Haemophilus influenzae secondary to acute otitis media. Serologic typing done by the state health department showed the strain to be nontypeable.
Figure 3. MALDI-TOF results
DISCUSSION
Haemophilus influenzae is a small, facultatively anaerobic, oxidase positive pleomorphic gram-negative rod. Of the standard media used for bacterial isolation, it grows only on chocolate agar, as it requires both factor X and factor V for growth1. On solid media, colonies are large, slightly opaque, colorless to grey, round, and smooth2. Haemophilus influenzae is broadly categorized into strains with a capsule, termed typeable, and those without, termed nontypeable. There are six typeable strains, serotype a through f, each with a unique capsule polysaccharide antigen. Each serotype can be detected serologically by agglutination using antisera specific to the unique polysaccharide antigen3.
Haemophilus influenzae can infect a variety of organs, and infection can be broadly categorized as invasive or non-invasive. Invasive infections are defined by tissue invasion beyond the mucosal surface and include clinical syndromes like meningitis, epiglottitis, pneumonia, cellulitis, endocarditis, osteomyelitis, septic arthritis, and bacteremia4. Invasive infections are associated with high mortality rates. Non-invasive infections include syndromes like acute otitis media, sinusitis, and conjunctivitis5. Haemophilus influenzae type b is by far the most virulent strain and, when infection occurs, has the highest propensity to cause invasive disease. Haemophilus influenzae type b used to cause the vast majority of invasive infections, however, widespread vaccination using the polysaccharide conjugate vaccine has drastically reduced cases6. As such, while rare, nontypeable Haemophilus influenzae now causes the majority of invasive infections7. Delayed treatment or treatment failure may allow an initially non-invasive infection to progress to invasive disease, as in this case.
Treatment of Haemophilus influenzae is most often empiric and beta-lactam antibiotics are usually used. Amoxicillin-clavulanate is a common choice for non-invasive infections, while intravenous cephalosporins, such as ceftriaxone, are common choices for invasive infections8. Of note, resistance to ampicillin, amoxicillin, and penicillin occurs relatively frequently now, usually due to production of beta-lactamases. Across the United States, approximately 25% of Haemophilus influenzae strains are beta-lactamase-producing9.
REFERENCES
![]() Contributed by Jacob Jerome, MD and William Pasculle, ScD
Contributed by Jacob Jerome, MD and William Pasculle, ScD