Diagnosis -- Mucoepidermoid Carcinoma, Low Grade with Oncocytic Features (with Cilia)
FINAL DIAGNOSIS
Mucoepidermoid Carcinoma, Low Grade with Oncocytic Features (with Cilia)
ANCILLARY STUDIES
MAML2 is positive for rearrangement by fluorescence in situ hybridization.
Figure 3.
DISCUSSION
Mucoepidermoid carcinoma (MEC) is the most common salivary gland malignancy and is histologically comprised of a mixture of mucous cells, intermediate cells and squamoid/epidermoid cells but may also demonstrate clear cell, oncocytic or columnar cells [1]. Approximately half of MECs occur in major salivary glands, predominantly in the parotid gland [2]. Most MECs harbor a tumor type-specific translocation at t(11;19)(q21;p13) expressing CRTC1::MAML2 fusion gene [2].
While most oncocytic MEC with lymphoid stroma (i.e. "Warthin like" MEC) raise Warthin tumor as a differential diagnostic consideration, here, given the attenuated almost single layered appearance of the majority of the lesion, lymphoepithelial cyst is a closer differential diagnostic consideration [3]. In contrast to this MEC, lymphoepithelial cyst tends to be more squamous, with only rare mucous cells. In lymphoepithelial cyst, the epithelium is often infiltrated by lymphocytes, rather than surrounded by sclerosis with lymphoplasmacytic infiltrates [4].
Cystadenoma of salivary gland is another entity in the differential diagnosis and may show a lining similar to that of this case. Although mucinous subtype is uncommon, it may mimic a purely cystic mucoepidermoid carcinoma. Cystadenomas, however, lack invasive growth and also lack complex arborizing and hierarchical papillary tufting [5]. Ciliated epithelium is not uncommon in MEC in our experience, and likely underreported given the recent interest in this topic, though it is only rarely prominent [6]. Thus, ciliated epithelium does not automatically equate to a benign diagnosis.
Finally, the impression of mucoepidermoid carcinoma was confirmed by our fluorescence in situ hybridization for MAML2 gene rearrangements.
Mucoepidermoid carcinomas are currently graded using a three-tiered system as: low, intermediate and high grade, based on a constellation of cytomorphologic and architectural features including cystic component, border, mitoses, anaplasia, perineural and angiolymphatic invasion among others [1].
Grading in mucoepidermoid carcinoma is important for prognosis and therapy. The reported 5-year overall survival rate for low grade MEC is 92-100%. Low grade MECs generally require only surgical treatment, while high grade MECs require adjuvant radiation and neck dissection [1].
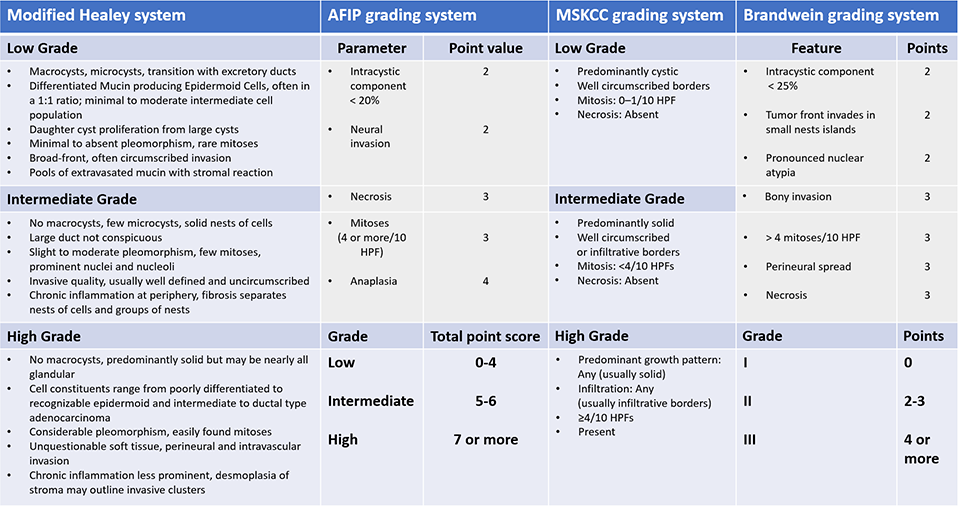
Different grading systems have been adopted for mucoepidermoid carcinomas and the four most popular grading systems are:
AFIP grading system [7]
Modified Healey system [8]
Brandwein system [9]
MSK Grading system [10] (Table [1])
Both the AFIP and Brandwein system are point-based, with each adverse histologic parameter being assigned a point value and higher scores equating to higher grades, while in the modified Healey and MSK grading system, a tumor is graded based on its predominant morphologic features with certain histologic parameters characterizing a particular grade. The MSK grading system shares some similarities with the modified Healey system in that it takes into account predominant growth pattern, but for high grade MEC criteria become more discrete (i.e. mitotic count and tumor necrosis).
The Brandwein grading scheme has been simplified to remove microstaging prognostically redundant parameters (angiolymphatic invasion, perineural invasion, bone invasion) and resolved to a simpler criteria based scheme with no adverse remaining parameters equating to low grade; one adverse to intermediate grade, and two or more adverse parameters to high grade.
The case presented here would be considered low grade by all commonly utilized grading systems and surgical excision would likely be curative.
MULTIPLE CHOICE QUESTIONS
1. The most common fusion occurring in mucoepidermoid carcinoma (MEC) is:
CRTC3::MAML2 fusion
CRTC1::MAML2 fusion
EWSR1::POU5F1 fusion
EWSR1::MAML2 fusion
Answer: B. Most MECs harbor a tumor type-specific translocation at t(11;19)(q21;p13) expressing CRTC1::MAML2 fusion gene. CRTC3::MAML2 fusion and EWSR1::POU5F1 fusion due to t(11;15)(q21;q26) translocation and t(6;22)(p21;q12), respectively, are seen in rare cases of MEC [11].
2. Which of the following is true:
CRTC1::MAML2 fusion may be seen in low, intermediate or high grade MECs
Low grade MECs show high-level copy number alterations
Low grade MECs typically show TP53 and/or POU6F2 somatic mutations
Answer: A. The CRTC1::MAML2 fusion is seen in most low and intermediate grade and some high grade tumors. Low grade MECs show minimal copy number variation and few somatic mutations, such as TP53 and POU6F2 [11].
3. Entities that enter the differential diagnosis of low grade MEC include:
Poorly differentiated squamous cell carcinoma
Salivary duct carcinoma
Warthin tumor with oncocytic or squamous metaplasia
Adenosquamous carcinoma
Answer: C. Entities with a bland cytomorphology, cystic and/or oncocytic appearance enter in the differential diagnosis of low grade MEC. These include: mucocele, necrotizing sialometaplasia, sclerosing sialadenitis with mucous metaplasia, pleomorphic adenoma and Warthin tumor with oncocytic or squamous metaplasia, sclerosing polycystic adenoma, cystadenoma, lymphoepithelial cyst and secretory carcinoma [11]. Squamous cell carcinoma, adenosquamous carcinoma and salivary duct carcinoma, on the other hand, can mimic high grade MEC.
4. Entities that enter the differential diagnosis of high grade MEC include:
Mucocele
Sclerosing sialadenitis with mucous metaplasia
Cystadenoma
Salivary duct carcinoma
Answer: D. Entities that have an oncocytic/apocrine appearance with a predominantly solid growth pattern, in addition to high grade histologic features, can mimic high grade MEC and include: carcinoma ex-pleomorphic adenoma, poorly differentiated SCC, adenosquamous carcinoma, salivary duct carcinoma and metastatic carcinomas [11]. Mucocele, sclerosing sialadenitis and cystadenoma, on the other hand, can mimic a low grade MEC.
5. Mucoepidermoid carcinomas of the head and neck most commonly occur in the:
Submandibular gland
Sublingual gland
Parotid gland
Palate
Mandible
Answer. C. Approximately half of MECs occur in major salivary glands, predominantly in the parotid gland, followed by the submandibular and the sublingual gland. Intraorally, the most common site is the palate followed by the buccal mucosa and other sites. Rare central MECs occur in the mandible or the maxilla [11].
REFERENCES
Seethala, R.R., An update on grading of salivary gland carcinomas. Head Neck Pathol, 2009. 3(1): p. 69-77.
Ilmo Leivo, J.A.B., Philippe Vielh, Hiroshi Inagaki, Nicole A. Cipriani, Valerie Costes-Martineau, Salivary Gland. Malignant epithelial tumours. Mucoepidermoid carcinoma., in WHO Classification of Tumours Editorial Board. Head and neck tumours, M.D.H. Alena Skalova, Ravi Mehrotra, Editor. 2022, Lyon (France): International Agency for Research on Cancer: [Internet; beta version ahead of print].
Garcia, J.J., et al., Fluorescence in situ hybridization for detection of MAML2 rearrangements in oncocytic mucoepidermoid carcinomas: utility as a diagnostic test. Hum Pathol, 2011. 42(12): p. 2001-9.
Juan C. Hernandez-Prera, P.E.W., Jr., Lisa M. Rooper, Brittany J. Holmes, Tumours and tumour-like lesions of the neck and lymph nodes. Cyst and cyst-like lesions. Lymphoepithelial cyst., in WHO Classification of Tumours Editorial Board. Head and neck tumours, M.D.H. Bruce M Wenig, Editor. 2022, Lyon (France): International Agency for Research on Cancer: [Internet; beta version ahead of print].
Abbas Agaimy, R.S., Roderick Howard, Wallace Simpson, Masato Nakaguro, Salivary Gland. Benign Epithelial tumours. Cystadenoma of salivary glands., in WHO Classification of Tumours Editorial Board. Head and neck tumours, M.D.H. Alena Skalova, Ravi Mehrotra, Editor. 2022, Lyon (France): International Agency for Research on Cancer: [Internet; beta version ahead of print].
Bishop, J.A., et al., MAML2 Rearrangements in Variant Forms of Mucoepidermoid Carcinoma: Ancillary Diagnostic Testing for the Ciliated and Warthin-like Variants. Am J Surg Pathol, 2018. 42(1): p. 130-136.
Goode, R.K., P.L. Auclair, and G.L. Ellis, Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria. Cancer, 1998. 82(7): p. 1217-24.
Batsakis, J.G. and M.A. Luna, Histopathologic grading of salivary gland neoplasms: I. Mucoepidermoid carcinomas. Ann Otol Rhinol Laryngol, 1990. 99(10 Pt 1): p. 835-8.
Brandwein, M.S., et al., Diagnosis and classification of salivary neoplasms: pathologic challenges and relevance to clinical outcomes. Acta Otolaryngol, 2002. 122(7): p. 758-64.
Katabi, N., et al., Prognostic features in mucoepidermoid carcinoma of major salivary glands with emphasis on tumour histologic grading. Histopathology, 2014. 65(6): p. 793-804.
Ilmo Leivo, J.A.B., Philippe Vielh, Hiroshi Inagaki, Nicole A. Cipriani, Valerie Costes-Martineau, Salivary Gland. Malignant epithelial tumours. Mucoepidermoid carcinoma., in WHO Classification of Tumours Editorial Board. Head and neck tumours, M.D.H. Alena Skalova, Ravi Mehrotra, Editor. 2022, Lyon (France): International Agency for Research on Cancer: [Internet; beta version ahead of print].
Contributed by Rayan Rammal, MD, and Raja Seethala, MD
)