FINAL DIAGNOSIS
Myelodysplastic syndrome with ring sideroblasts and thrombocytosis
DISCUSSION
The bone marrow specimen is hypercellular with trilineage hematopoiesis. Megakaryocytes are increased, with some clustering noted and some atypical forms. Iron stain demonstrates a moderate number of ring sideroblasts. Dyserythropoiesis is present. With the patient's normocytic anemia and thrombocytosis, a primary differential diagnostic consideration is myelodysplastic/myeloproliferative neoplasm with ring sideroblasts and thrombocytosis (MDS/MPN-RS-T). Additional molecular studies, karyotyping, and fluorescence in-situ hybridization (FISH) studies are necessary to rule out other myelodysplastic syndromes and myeloproliferative neoplasms.
Cytogenetic and molecular studies are performed on the specimen. The karyotype is normal (46 XX), microarray studies show no abnormalities, and BCR-ABL1 translocation is not detected by FISH analysis. Next-generation sequencing for genomic alterations demonstrate pathogenic mutations in SF3B1 (p.Lys700Glu and p.His662Asp), ASXL1, and TET2. Mutations in SF3B1 support the diagnosis of MDS/MPN-RS-T, and there are no genomic alterations identified that would alter the diagnosis.
Myelodysplastic syndrome/myeloproliferative neoplasm with ring sideroblasts and thrombocytosis (MDS/MPN-RS-T) falls in the category of overlapping myelodysplastic/myeloproliferative neoplasms. The defining criteria include thrombocytosis (![]() 450 × 109/L), < 1% blasts in the peripheral blood, ring sideroblasts accounting for
450 × 109/L), < 1% blasts in the peripheral blood, ring sideroblasts accounting for ![]() 15% of erythroblasts, dyserythropoiesis, and < 5% blasts in the bone marrow [1]. This overlapping condition must be differentiated from the myelodysplastic syndromes (such as myelodysplasia with ring sideroblasts), the myeloproliferative neoplasms (such as essential thrombocytosis), and non-clonal conditions with ring sideroblasts (such as congenital diseases of mitochondrial dysfunction). In MDS/MPN-RS-T, the red blood cells may demonstrate two distinct populations accompanying increased platelets, often ranging in size. Bone marrow often shows megaloblastoid or dyserythropoietic characteristics in the erythroid precursors, as well as large, hyperlobated megakaryocytes [1]. Approximately 80% of cases of MDS/MPN-RS-T have a SF3B1 mutation, which is associated with a JAK2 p.Val617Phe mutation in more than 50% of cases overall. Rarely, SF3B1 mutations are associated with CALR or MPL mutations [2].
15% of erythroblasts, dyserythropoiesis, and < 5% blasts in the bone marrow [1]. This overlapping condition must be differentiated from the myelodysplastic syndromes (such as myelodysplasia with ring sideroblasts), the myeloproliferative neoplasms (such as essential thrombocytosis), and non-clonal conditions with ring sideroblasts (such as congenital diseases of mitochondrial dysfunction). In MDS/MPN-RS-T, the red blood cells may demonstrate two distinct populations accompanying increased platelets, often ranging in size. Bone marrow often shows megaloblastoid or dyserythropoietic characteristics in the erythroid precursors, as well as large, hyperlobated megakaryocytes [1]. Approximately 80% of cases of MDS/MPN-RS-T have a SF3B1 mutation, which is associated with a JAK2 p.Val617Phe mutation in more than 50% of cases overall. Rarely, SF3B1 mutations are associated with CALR or MPL mutations [2].
The prognosis of MDS/MPN-RS-T is generally good, with a median overall survival of 76-128 months [2]. Independent prognostic factors for overall survival include age, presence of a SF3B1 mutation, and presence of JAK2 p.V617F mutation, where younger patients with both mutations have the best overall outcomes. Treatment regimens for MDS/MPN-RS-T are adapted from those for MDS and MPN, with no well-established treatment regimens. Treatment is often based on the presenting patient problem, with anemic symptoms treated similarly to lower risk MDS (erythropoiesis stimulating agents and transfusion support) and risk of thrombotic events treated similarly to essential thrombocytosis (combination of aspirin and observation or hydroxyurea for cytoreduction) (Figure 2) [2]. However, a case study of treatment with single agent lenalidomide reported positive outcomes [3]. Patients with MDS/MPN-RS-T are also at risk for migraine headaches, palpitations, paresthesia, chest pain, or acquired von Willebrand's disease.
Ring sideroblasts are erythroid precursors that have an abundance of iron located within the mitochondria. Iron granules are identified using Prussian blue staining (Perls' reaction). The defining criteria of a ring sideroblast requires that an erythroblast has at least 5 siderotic granules encompassing at least a third of the nuclear circumference [4]. These pathologic cells are different than ferritin sideroblasts, which are non-pathologic sideroblasts that contain scattered iron granules within endosomes in the cytoplasm. Ring sideroblasts may be identified in MDS-RS, MDS/MPN-RS-T, X-linked sideroblastic anemia (mutations in ALAS2), autosomal recessive congenital sideroblastic anemia (mutations in SLC25A38, GLRX5, HSPA9, HSCB, or FECH), X-linked sideroblastic anemia and ataxia (mutations in ABCB7), MLASA (myopathy, lactic acidosis and sideroblastic anemia caused by mutations in IARS2, LARS2, MT-ATP6, NDUFB11, PUS1, or YARS2 genes), SFID (sideroblastic anemia, B cell immunodeficiency, periodic fevers, and developmental delay caused by mutations in TRNT1), thiamine-responsive megaloblastic anemia (mutation in SLC19A2), and Pearson marrow-pancreas syndrome (mitochondrial DNA deletion) [5]. Many of the congenital conditions with ring sideroblasts are mechanistically related through mitochondrial dysfunction. Ring sideroblasts may also be seen due to excess alcohol use, medication use (isoniazid, chloramphenicol, linezolid, or chemotherapies), hypothermia, or copper deficiency.
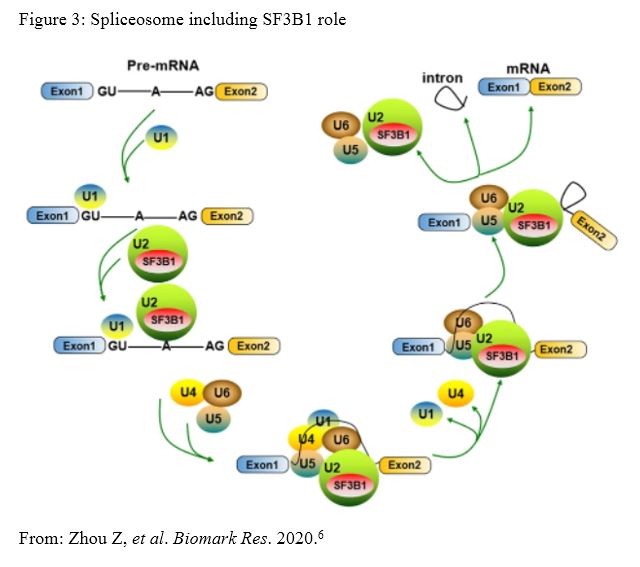
SF3B1 mutations are found in approximately 80% of cases of MDS/MPN-RS-T. The gene codes for the splicing factor 3b subunit 1 molecule which is a member of the spliceosome. The spliceosome is a complex made up of snRNAs and proteins that combine to form snRNPs. The snRNPs then complex to form a catalyst for mRNA transcript splicing event. SF3B subunits are present in each snRNP and play a role in the recognition and selection of the branch site for splicing. SF3B1 is the largest subunit of the SF3B complex and makes up part of the U2 snRNP (Figure 3) [6]. The most common mutation in SF3B1 is at p.Lys700Glu, which accounts for more than 50% of pathogenic mutations. Other hotspots include codons p.Lys666, p.His662, p.Glu622, and p.Arg625 [6]. SF3B1 mutations are present in many hematolymphoid conditions, including MDS (approximately 30% of patients), MDS-RS (approximately 80% of patients), MDS/MPN (approximately 20% of patients), and chronic lymphocytic leukemia (CLL) (approximately 15% of patients) [6]. In solid tumors, SF3B1 mutations have been found in multiple types of melanoma, neuroblastoma, pancreatic ductal adenocarcinoma, prostate cancer, and estrogen-receptor-positive breast cancer. Studies suggest that malignancies with SF3B1 mutations have better overall survival in some cases, but other studies found no significant effect on clinical outcomes. SF3B1 mutations have been shown to have a good prognosis in MDS and uveal melanoma (at least initially), but mutated SF3B1 has a poorer prognosis in CLL.
REFERENCES
![]() Contributed by Jeff Kleinberger, MD, PhD and Bryan Rea, MD
Contributed by Jeff Kleinberger, MD, PhD and Bryan Rea, MD