![]() Contributed by Aofei Li, MD, Changqing Ma, MD. PhD, Michael Landau, MD, Octavia M. Peck-Palmer, PhD
Contributed by Aofei Li, MD, Changqing Ma, MD. PhD, Michael Landau, MD, Octavia M. Peck-Palmer, PhD
CLINICAL HISTORY
The patient is a gentleman in his 60s with a clinical history of chronic pulmonary disease, status post double lung transplant and receiving tacrolimus, prednisone, and prophylactic valganciclovir treatments. He presented with recurrent epigastric to diffuse abdominal pain, nausea, vomiting and bouts of watery diarrhea for three months. CT imaging study demonstrated small bowel wall thickening and fat stranding concerning for duodenitis.
Upper endoscopy findings
Small bowel enteroscopy showed esophageal mucosal changes suspicious for short-segment Barrett's esophagus, erosive gastropathy in the antrum, and duodenal erosions. Biopsies were taken from the distal esophagus, stomach, and duodenum. The endoscopic picture of distal esophagus is shown in Figure 1A. Photomicrographs of the routine Hematoxylin and Eosin (H&E) stained tissue sections of the esophageal biopsies are shown in Figure 1B-C. Immunohistochemistry for a certain virus performed on the esophageal biopsy is shown in Figure 1D. Biopsy of small bowel and stomach demonstrated similar findings.
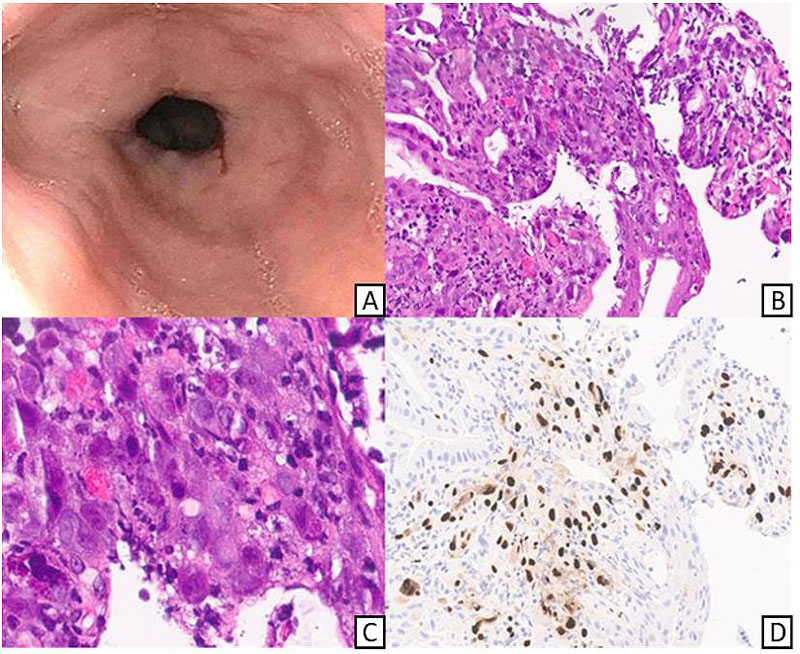
Figure 1. Esophageal findings. A: Endoscopic image of gastro-esophageal junction with abnormal mucosa. B, C: esophageal biopsy showing cytopathological changes (H&E stain, 200x and 400x, respectively, cropped digital image) D: Immunohistochemical stain for the culprit virus (200x, cropped digital image)
Virology studies
The patient's clinical course was complicated by refractory viremia of the same virus. The patient also received virus-specific cytotoxic T-cell infusion at an outside hospital (Figure 2).
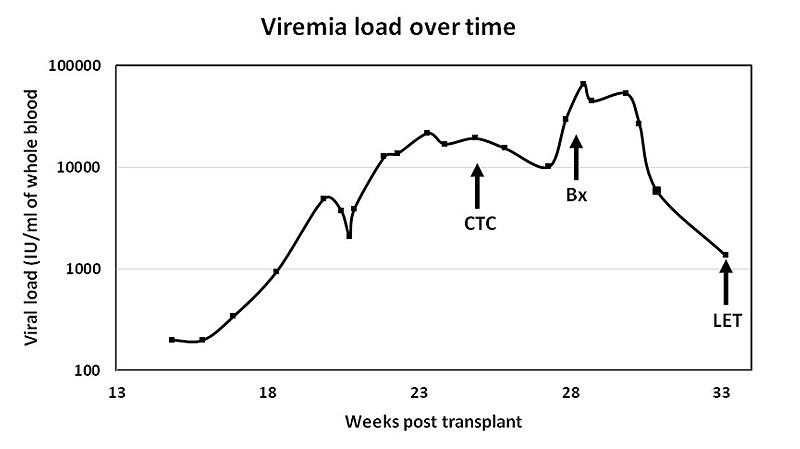
Figure 2. Viremia load over the patient's clinical course. "CTC" indicates the time of cytotoxic T cell infusion. "Bx" indicates the time of esophageal biopsy. "LET" indicates the time of letermovir therapy.
Antiviral resistance study found both wild-type and A594V mutation at the UL97 locus of the viral genome suggesting a mixed viral population. UL54 locus mutations were negative.