FINAL DIAGNOSIS:
DISCUSSION:
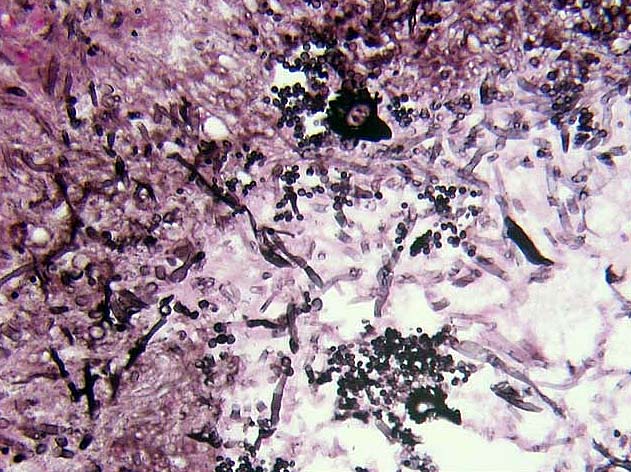
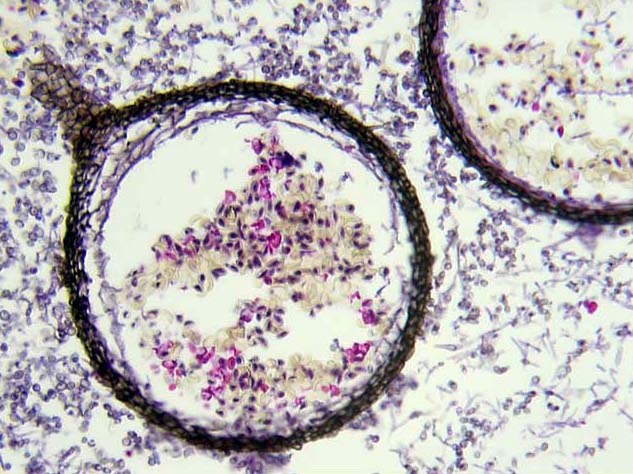
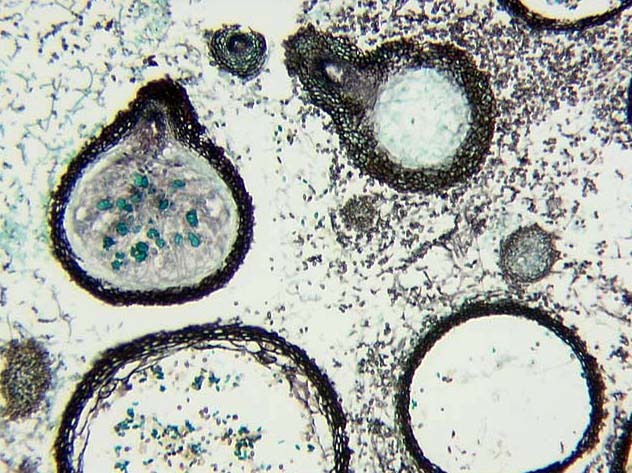
Phaeohyphomycosis is a collective term for a heterogeneous group of mycotic infections that contain dematiaceous (dark pigment producing) yeast-like cells, pseudohyphae-like elements, hyphae, or any combination of these forms in tissue.1 Sinusitis is a common form of clinical infection with phaeohyphomycotic fungi which are saprobic (meaning they derive nutrient from dead organic matter). Cases of dematiaceous fungal sinusitis reported in the literature include species of Bipolaris,2 Exserohilum,3 Curvularia,4 Alternaria4 and Microascus.5,6 Speciation of these fungi often require successful cultivation of organisms on nutrient agar for visualization of the most specific morphologies exhibited by the various species. Sexual (teleomorph) and asexual (anamorph) forms of the organisms further complicate the nomenclature as different designations have been given to these morphologic forms of the same organism, e.g. Pseudoallesheria boydii (teleomorph) and Scedosporium apiospermium (anamorph). The sexual forms exhibited by fungi are further broadly divided by the final location of mature spores in relation to the modified "parent" hyphae. Ascospores are contained within an ascus while basidiospores are borne external to a basidium. The ascomycetous species may also produce a fruiting body called an ascocarp or ascoma that covers the naked asci that contain the ascospores and are also utilized to classify organisms by five general morphologic types of ascocarps. One type referred to as a cleistothecium is global in shape with a wall (peridium) formed of pseudoparenchymatous hyphae. Human pathogens that produce cleistothecium include P. boydii, Emericella nidulans (anamorph is Aspergillus nidulans) and Microascus sp. (the sexual form for some Scopulariopsis sp.).
As this case illustrates, it could prove useful for the neuropathologist to be aware of the diverse morphologic forms fungi can exhibit as the clinical history presented is not particularly unusual. While the pigment production and ascomata with a cylindrical or tapering beak were enough to narrow the fungi identity in this case to a Microascus sp. without successfully cultivating the organism, Pseudoallasheria was certainly in our differential. This differential is important as Pseudoallasheria sinusitis has been reported in both AIDS patients7 and nonimmunocompromised host with intracranial extension.8 This is significant for the fact that Pseudoallasheria boydii is known to be resistant to amphotericin B while remaining susceptible to miconazole antifungal therapy.7,8 The patient presented in this case was treated with amphotericin B out of concern that the risk of intracranial extension of this fungal sinusitis would be greater status post transnasal endoscopic resection of his pituitary adenoma. While intravenous amphotericin B is the recommended treatment for phaeohyphomycotic paranasal sinusitis9 and has been used successfully in treating a pediatric bone marrow transplant recipient with cutaneous and pulmonary infection by Microascus cirrosus,6 we find no reported cases in the literature of intracranial extension from phaeohyphomycotic paranasal sinusitis due to Microascus sp. In January, 1998 he received gamma knife radiosurgery for residual progressive pituitary adenoma and exhibits no evidence of fungal infection clinically.
REFERENCES:
![]() Contributed by Charles A. Richert, M.D., John E. Sheaffer, Hae Dong Jho, M.D. and Ronald L. Hamilton, M.D.
Contributed by Charles A. Richert, M.D., John E. Sheaffer, Hae Dong Jho, M.D. and Ronald L. Hamilton, M.D.
{kind=link}
{kind=link}
{kind=link}