![]() Contributed by Azfar Neyaz, MD, and Steven F. Dobrowolski, PhD
Contributed by Azfar Neyaz, MD, and Steven F. Dobrowolski, PhD
CLINICAL HISTORY
A 3-day-old male newborn was brought to the outside hospital (OSH) emergency department by his mother with complaints of poor feeding, lethargy, and excessive sleep.
The baby was born at 41 weeks of gestation through a caesarian section following fetal bradycardia. The immediate postnatal course was uneventful; the child weighed 3.03 kg (borderline small for gestational age) and was phenotypically normal except failed hearing screening test on one ear. The mother (22 years, G1P1) had an uncomplicated antenatal course with no history of smoking, alcohol intake, or illicit drug usage. There was no history of gestational diabetes. Family history is non-contributory. Hepatitis B vaccine was given at birth, and he was exclusively breastfed. Mother and newborn were discharged with standard postnatal care instructions.
The child appeared irritable, hypothermic (91.5 F), and mildly dehydrated; the remaining metrics of the physical examination were unremarkable. Clinical suspicion of sepsis was raised. Laboratory workup revealed severe hypoglycemia (< 20 mg/dL) and lactic acidosis (4.4 mmol/L). Three 10% dextrose boluses were given, followed by 10% dextrose maintenance infusion to maintain blood glucose levels between 120-170 mg/dL.
The patient was transferred to the CHP NICU, where he underwent multiple evaluations for these symptoms, including sepsis workup, which was negative. The complete laboratory workup is detailed in Table 1.

An abnormal newborn screening (NBS) report came back shortly after arrival to the CHP NICU with increased concentrations of octanolycarnitine (C8=29.9 µmol/L, NR- 0.3-0.01), hexanolycarnitine (C6=3.74 µmol/L, NR- 0.2-0.01), decanoylcarnitine (C10 =1.58 µmol/L, NR -0.4-0.05) (Table 2).
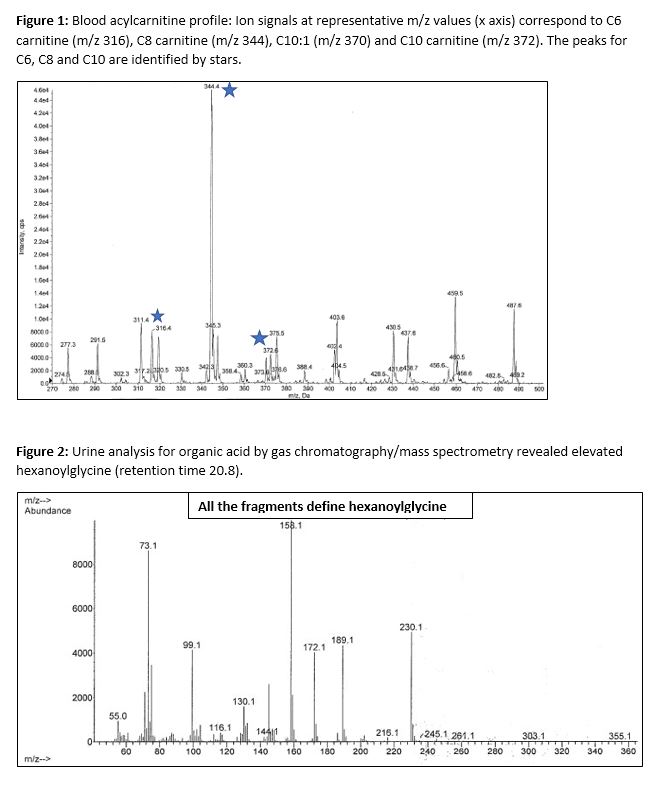
In response to abnormal NBS result, blood acylcarnitine profile was performed at CHP, using tandem mass spectrometry, showing significantly elevated concentrations of C8 (6.3 µmol/L), along with relatively higher levels of C6 (1.2 µmol/L), C10 (0.67 µmol/L) and C10:1 (0.57 µmol/L) (Figure 1); result consistent with the newborn screening test result. Urine organic acid analysis by gas chromatography/mass spectrometry revealed an over-representation of hexanoylglycine (Figure 2). Serum carnitine levels were within the normal range. MRI brain assessment was unremarkable and endocrine workup was within normal range
Molecular genetic testing showed compound heterozygote for c.985A>G (p.K329Q) and c.199T>C (p.Y67H) pathogenic variants of ACADM gene.